Chapter 2: Osteology
Anthropology is the study of people, and the skeleton is the framework of the person. So while all subdisciplines of anthropology study human behavior (culture, language, etc.) either presently or in the past, biological anthropology is the only subdiscipline that studies the human body specifically. And the fundamental core of the human (or any vertebrate) body is the skeleton. Osteology, or the study of bones, is central to biological anthropology because a solid foundation in osteology makes it possible to understand all sorts of aspects of how people have lived and evolved.1
ANATOMICAL TERMINOLOGY
Scientists have adopted standardized terminology to describe the position of the body as well as the location and movements of different body parts relative to one another. Below you will find descriptions of standard anatomical position, directional terms, anatomical planes, and skeletal movements (i.e., movements possible where two bones articulate through a joint).1
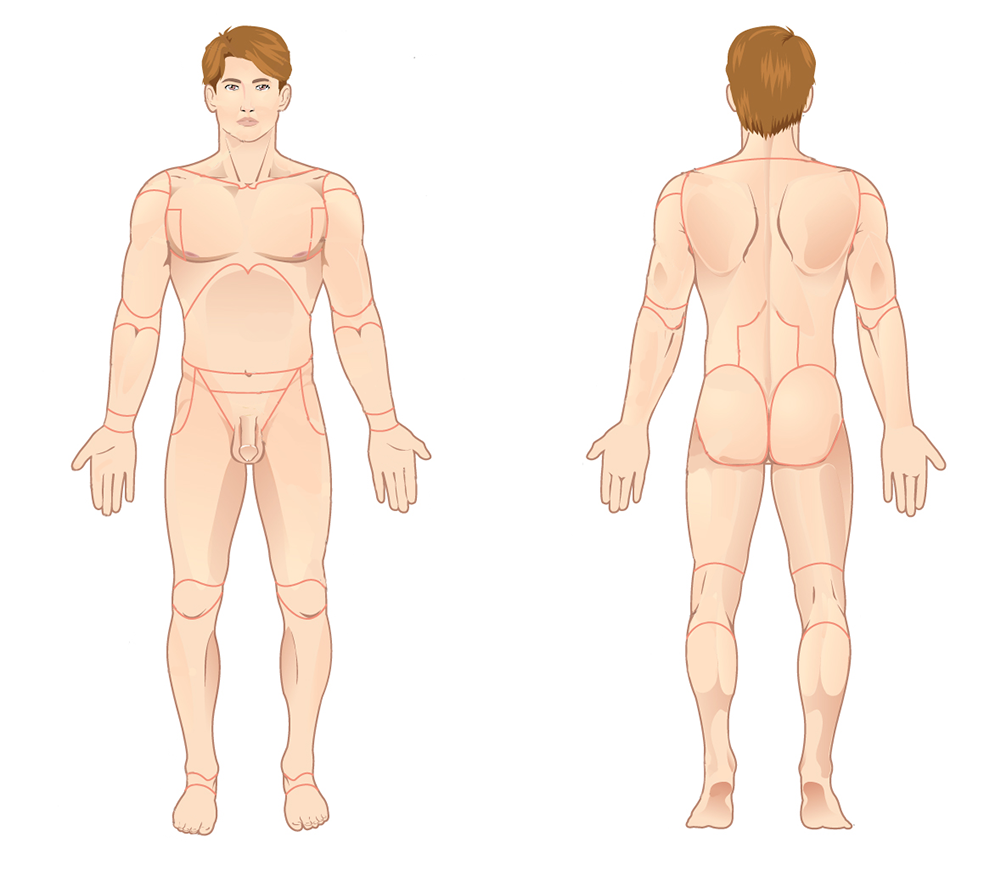
When a body is in anatomical position, it is situated as if the individual is standing upright; with head, eyes, and feet pointing forward (anteriorly, see below); and with arms at the side and palms facing forward. In anatomical position, the bones of the forearm are not crossed (Figure A.1).1
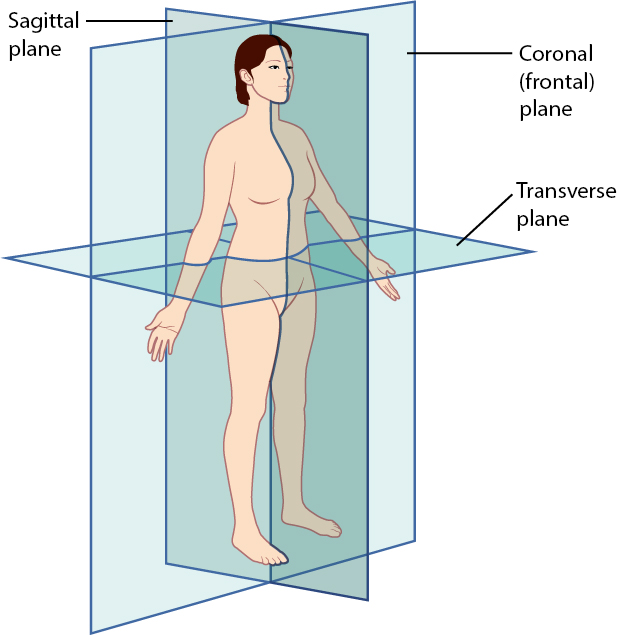
With the body in anatomical position, the position of specific organs (e.g., bones) can be described as situated within specific anatomical planes (Figure A.2). These imaginary planes bisect the body into equal or subequal halves, depending on which plane is described. Coronal (frontal) planes divide the body vertically into anterior (front) and posterior (back) halves. Transverse planes divide the body horizontally into superior (upper) and inferior (lower) halves. Sagittal planes divide the body vertically into left and right halves. The plane that divides the body vertically into equal left and right halves is called the midsagittal plane. The midsagittal plane is also called the median plane because it is in the midline of the body. If the left and right halves of the body are divided unequally (i.e., the right “half” is larger than the left “half” or vice versa), we call that dividing plane a parasagittal plane. There are potentially an infinite number of parasagittal planes that can be drawn to divide the body into unequal right and left “halves.”1
Directional Terms
When describing the position of one body part (in this case, a bone) relative to another, scientists use precisely defined directional terms. Each of the directional terms described below refers to the body in anatomical position. This is an important point because once the position of one bone is established relative to another, that directional term is the same, regardless of whether the body remains in anatomical position (e.g., the skull is always superior to the vertebrae, even if the individual is lying down).1
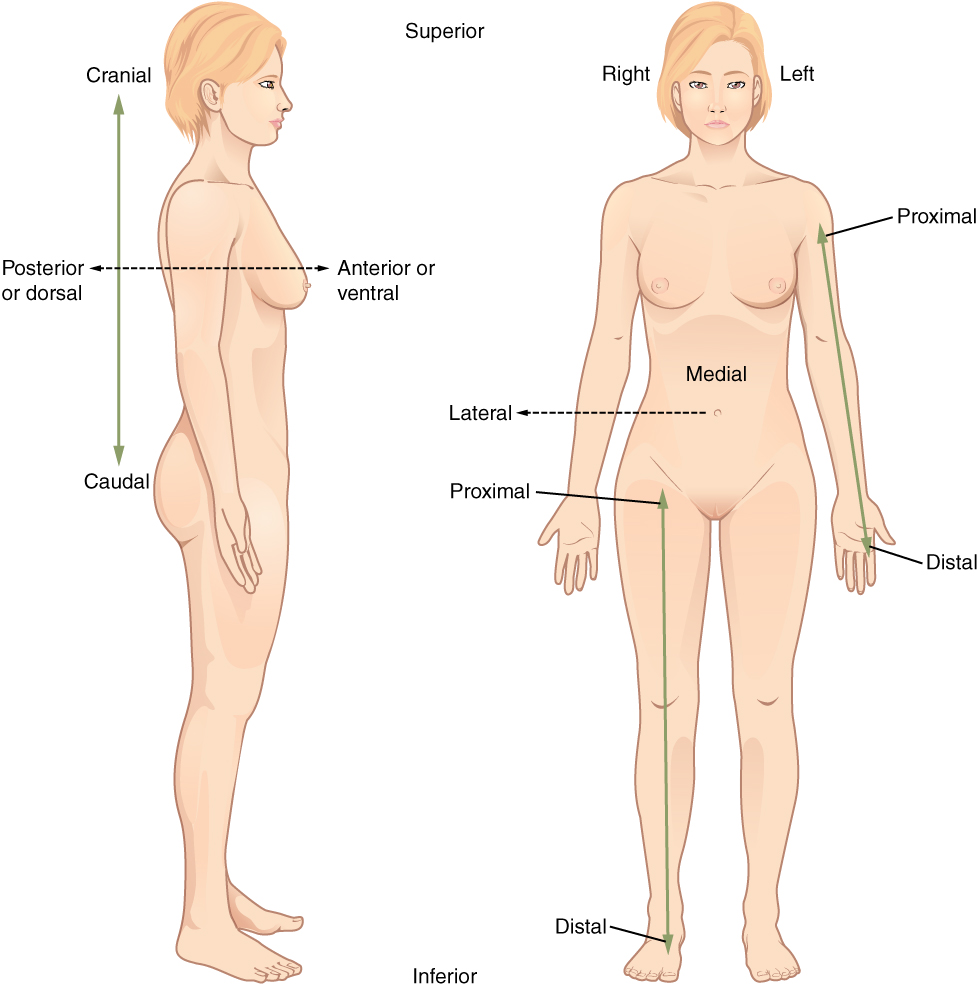
A bone or skeletal feature that is anterior (or ventral) is located toward the front of the body and a bone that is posterior (or dorsal) is located toward the back of the body (Figure A.3). For example, the sternum (breastbone) is anterior to the vertebral column (“backbone”). A medial bone is located closer to the midline (midsagittal plane) than a bone that is lateral, or located further from the midline. For example, the thumb is lateral to the index finger. A structure that is proximal is closer to the trunk of the body (usually referring to limb bones) than a distal structure, which is further from the trunk of the body. For example, the femur (thigh bone) is proximal to the tibia (leg bone). Finally, structures that are superior (or cranial) are located closer to the head than structures that are inferior (or caudal). For example, the rib cage is superior to the pelvis, and the foot is inferior to the knee. Typically, the terms “cranial” and “caudal” are used in reference to the non-human, quadrupedal skeleton, whereas “superior” and “inferior” are used in reference to the human skeleton.1
SKELETAL FORM AND FUNCTION
Structure and Material of Bone
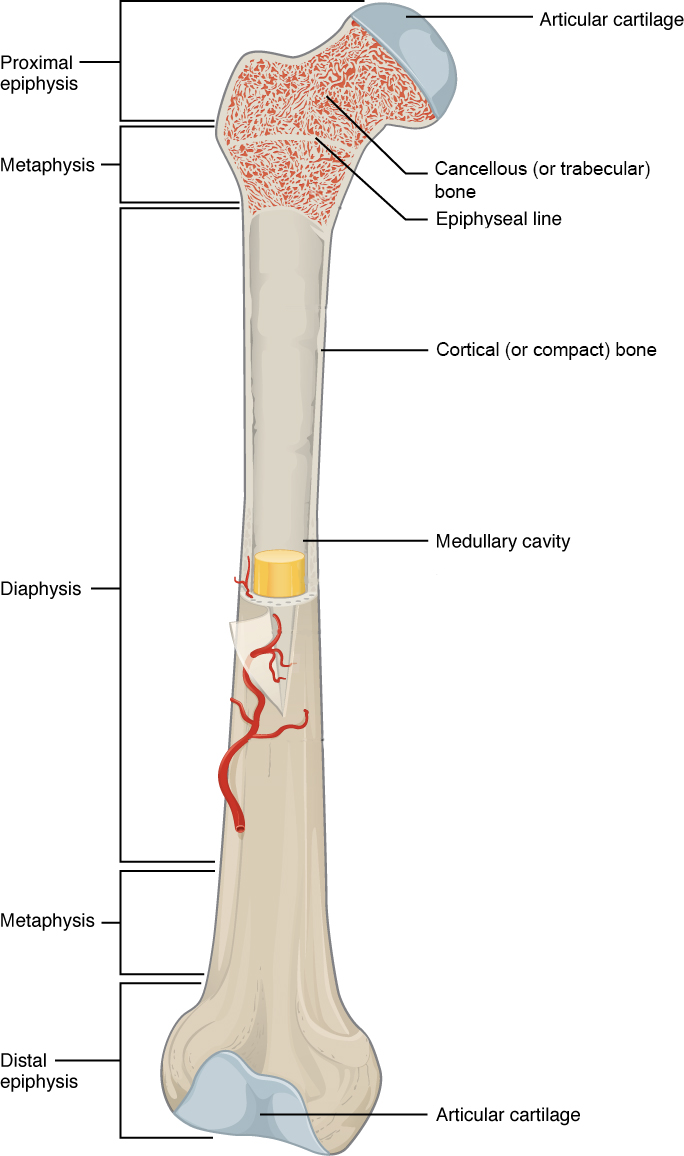
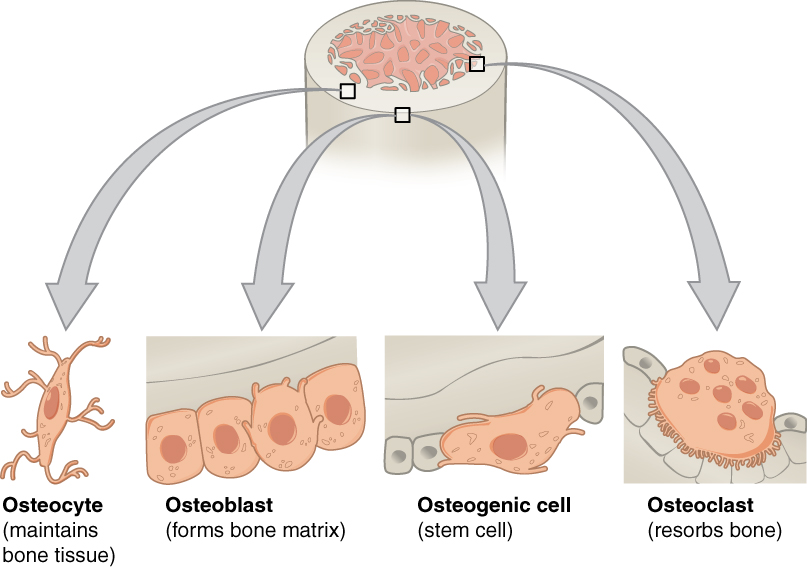
Bone is a composite of organic (collagen) and inorganic (mineral, e.g., hydroxyapatite, a calcium phosphate salt) materials with incredible strength in compression so it can support the body under the force of gravity. When bone is mature (fully mineralized as opposed to juvenile and undermineralized), it comprises an outer dense region of bone called cortical (or compact) bone and an inner spongy region of bone called cancellous (or trabecular) bone (Figure A.4). However, the interfaces between the organic and inorganic materials, as well as the cortical and cancellous regions, are subject to changing stresses. Each time we move our muscles, our bones are subjected to a combination of bending, twisting, compression, and tension. This results in the formation of microscopic cracks that weaken the bone and may result in complete bone fracture. Bone cells called osteocytes have special properties that allow them to sense when these microcracks form. Osteocytes then signal osteoclast cells to remove the cracked bone and osteoblast cells to lay down new bone—a process known as skeletal remodeling. Osteogenic cells are stem cells that are able to differentiate into osteoblasts (Figure A.5).1
Bone Shape
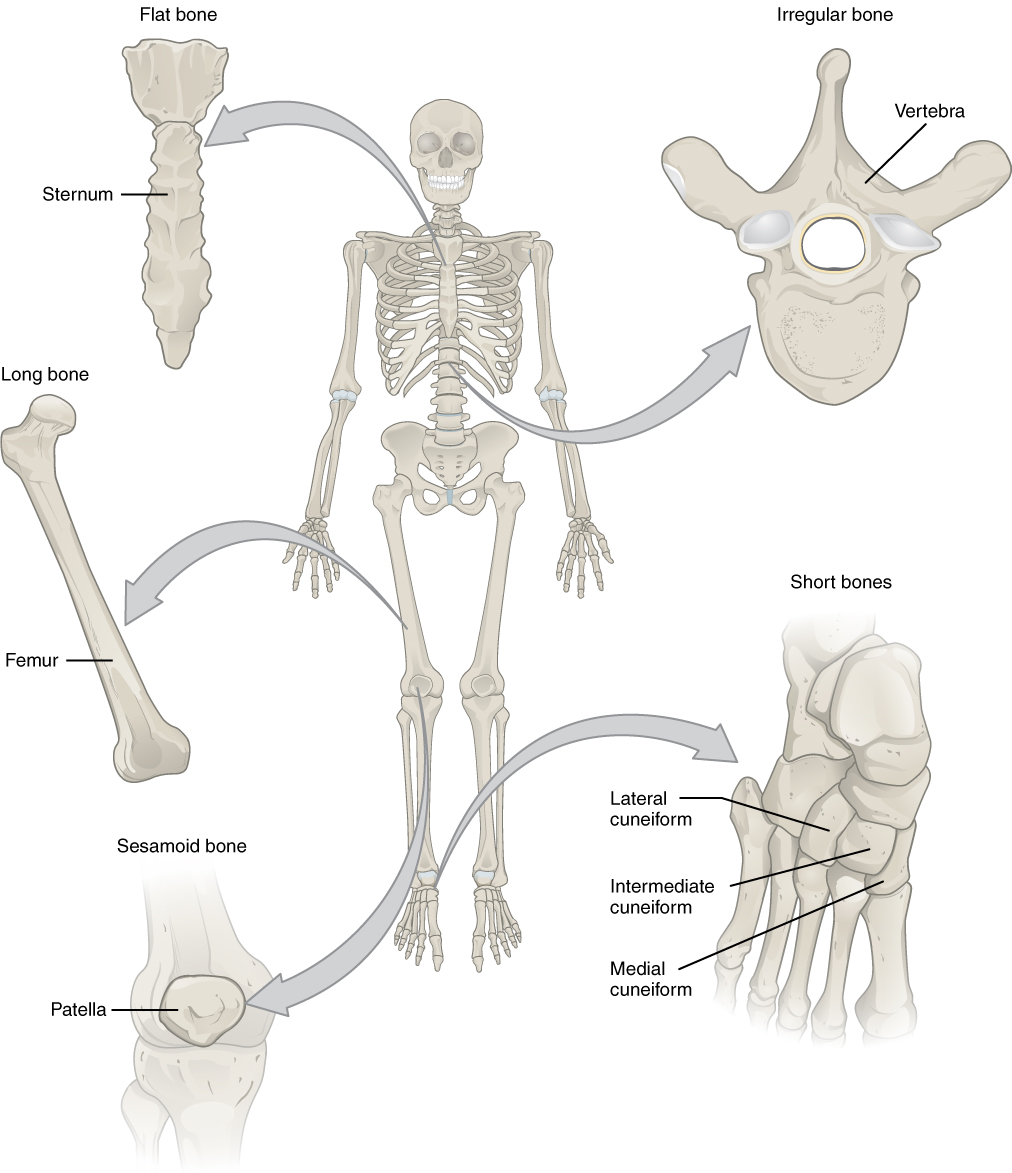
Different bones have different shapes that largely relate to their specific function within the skeletal system. Additionally, the ratio of cortical to cancellous bone, and which muscles are attached to the bone and how, affect the shape of the whole bone. Generally there are five recognized bone shapes: long bones, short bones, flat bones, sesamoid bones, and irregular bones. Long bones are longer than they are wide and consist of three sections: diaphysis, epiphysis, and metaphysis (Figure A.4). The diaphysis of a long bone is simply the shaft of the bone, and it comprises mostly cortical bone with a thin veneer of internal cancellous bone lining a medullary cavity. At both the proximal and distal ends of every long bone, there is an epiphysis, which consists of a thin shell of cortical bone surrounding a high concentration of cancellous bone. The epiphysis is usually coated with hyaline (or articular) cartilage to facilitate joint articulation with other bones. The junction between diaphysis and epiphysis is the metaphysis, which has a more equal ratio of cortical to cancellous bone. Examples of long bones are the humerus, the femur, and the metacarpals and metatarsals.1
The other bone shapes are simpler. Short bones are defined as being equal in length and width, and they possess a mix of cortical and cancellous bone (Figure A.6). They are usually involved in forming movable joints with adjacent bones and therefore often have surfaces covered with hyaline cartilage. Examples of short bones are the carpals of the wrist and the tarsals of the ankle.1
Flat bones, as their name suggests, are flat and consist of two layers of thick cortical bone with an intermediate layer of cancellous bone called a diploe. Examples of flat bones are most of the bones of the skull, such as the frontal and parietal bones, as well as all parts of the sternum (Figure A.6). Sometimes bones develop within the tendon of a muscle in order to reduce friction on the joint surface and to increase leverage of the muscle to move a joint. These types of bones are called sesamoid bones, and these include the patella (or knee cap) and the pisiform (a bone of the wrist).1
Irregular bones are bones that don’t fit into any of the other four categories. The shapes of these bones are often more complex than the others, and examples include the vertebrae and certain bones of the skull, like the ethmoid and sphenoid bones (Figure A.6).1
Bone Formation
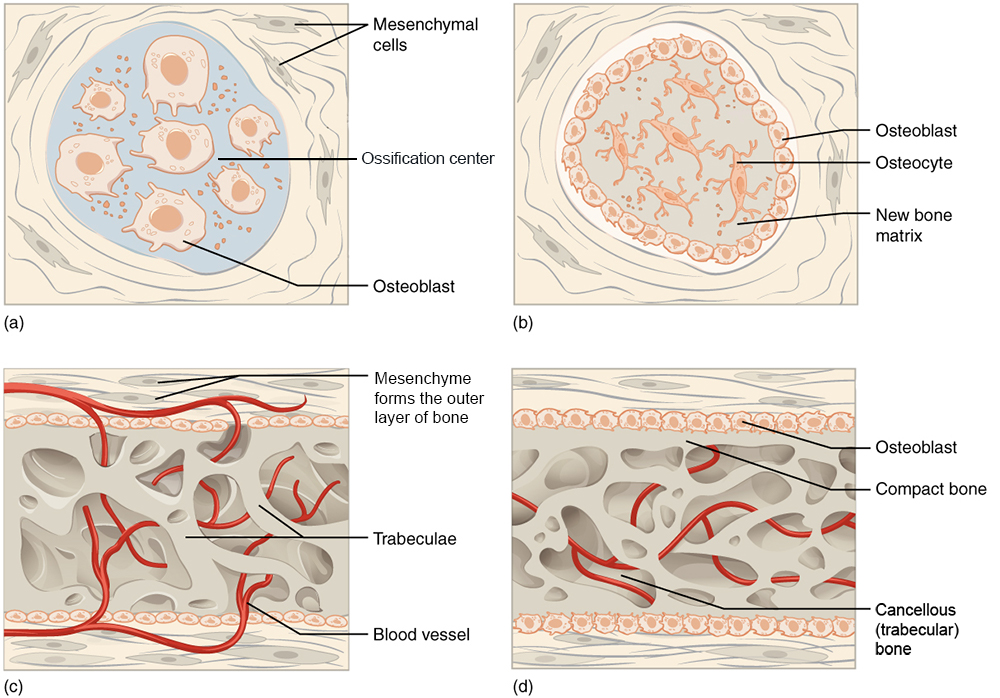
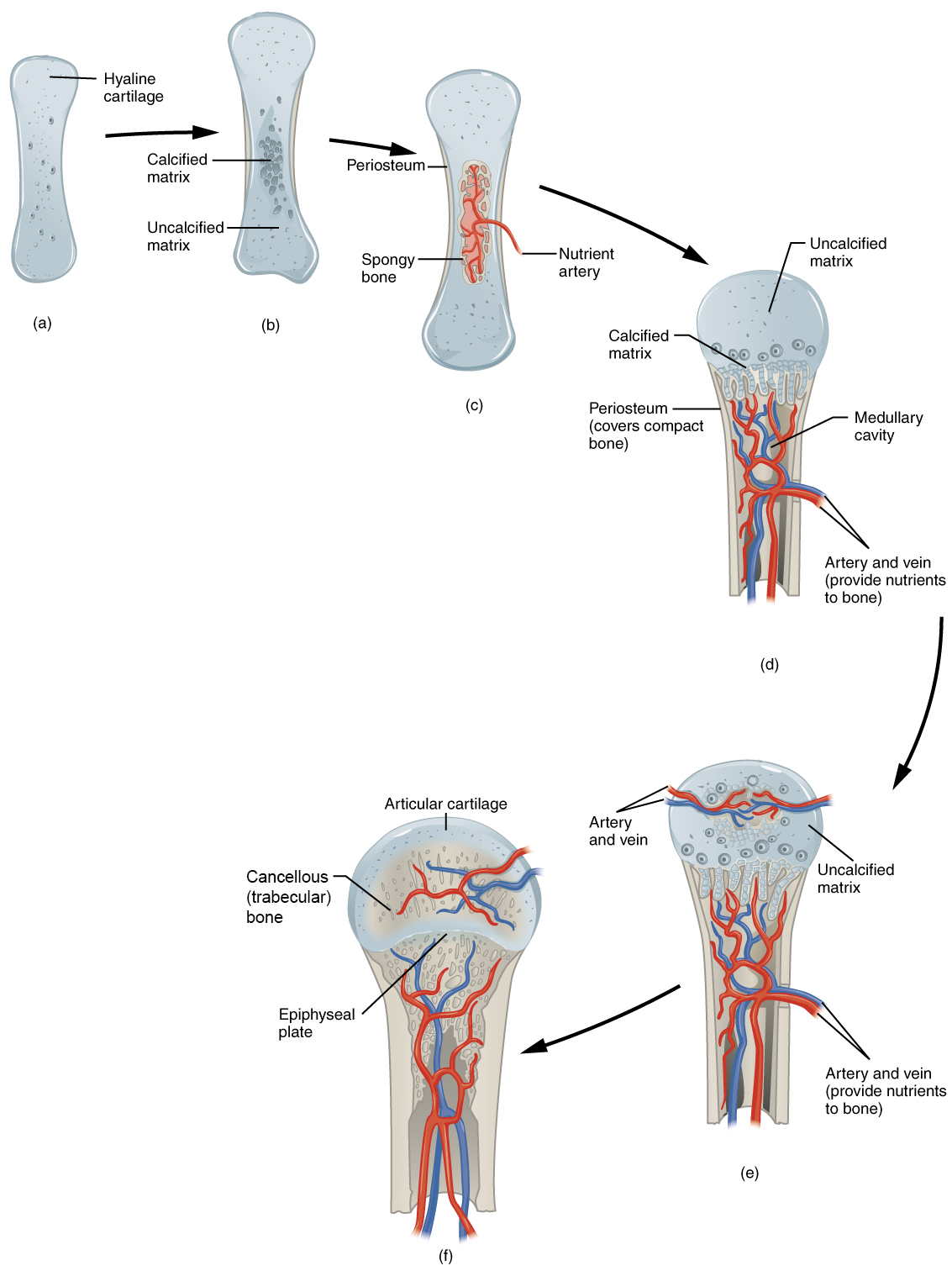
Bone develops via one of two mechanisms: intramembranous or endochondral bone formation. Intramembranous bone formation occurs when connective tissue mesenchymal (stem) cells aggregate and differentiate into osteoblasts, which then begin to synthesize new bone along the aggregated connective tissue cells (Figure A.7). Intramembranous bone formation is the mechanism by which most bones of the skull develop as well as the clavicle (collar bone). When osteoblasts develop from an intermediate cartilage “model” that is then replaced by bone, instead of developing directly from the mesenchymal cells, the mechanism is described as endochondral bone formation (Figure A.8). Endochondral bone formation is the mechanism by which most bones of the skeleton develop.1
Bone Function
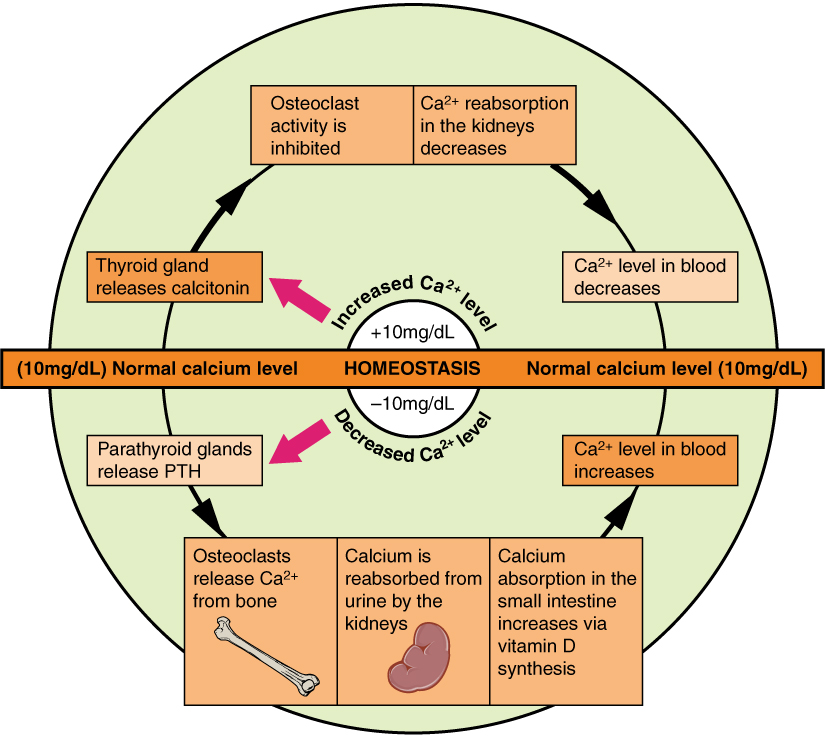
Bone performs both metabolic and mechanical functions for the body. On the metabolic side, bone is required to maintain mineral (i.e., calcium) homeostasis and for the production of red and white blood cells (Figure A.9), which develop in the cavity and the cancellous region of the metaphysis and epiphysis. But it is undeniable that the mechanical functions of bone are primary because bone is critically responsible for protecting internal organs, providing support against the force gravity, and serving as a network of rigid levers for muscles to act upon during movement.1
HUMAN SKELETAL SYSTEM
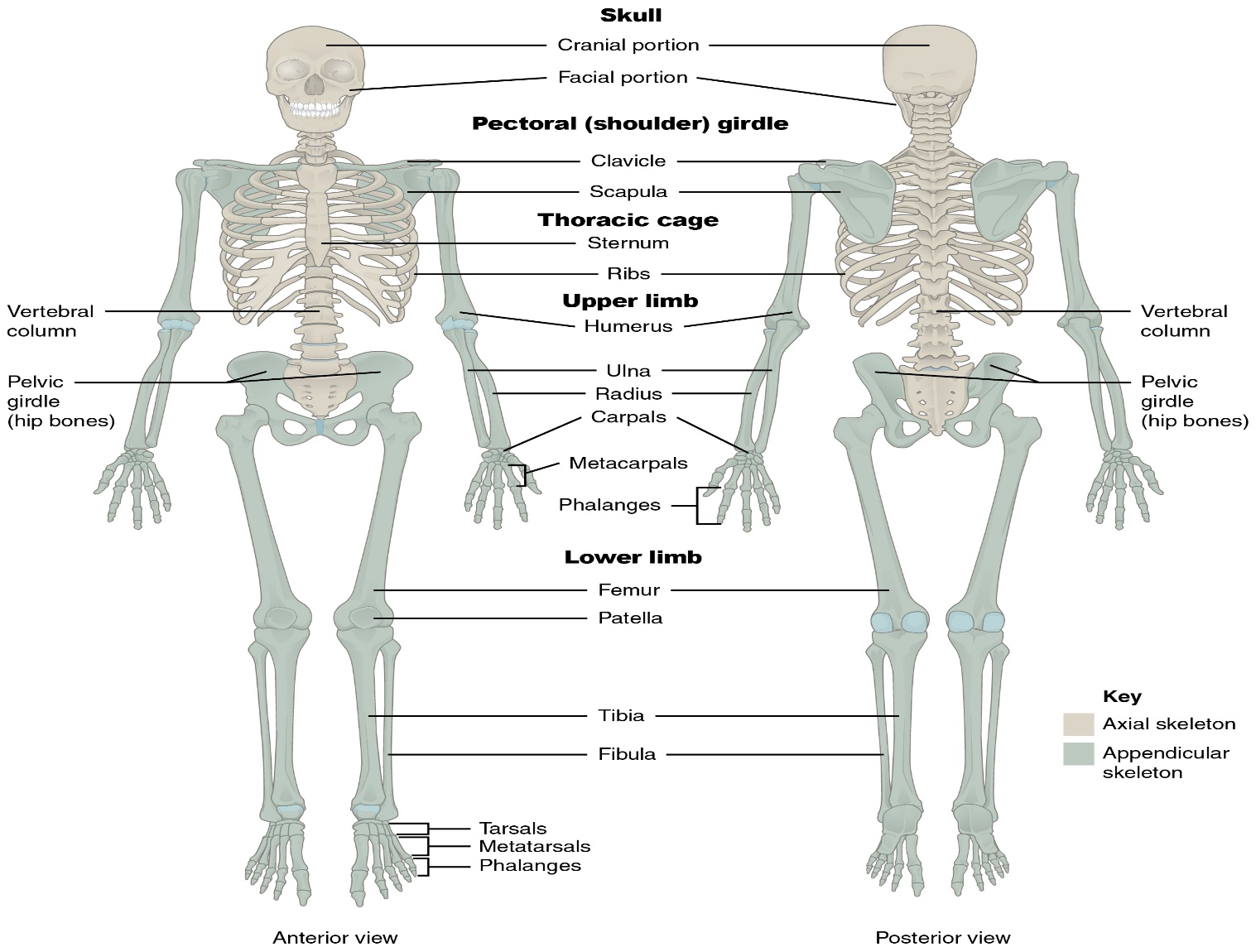
The skeletal system is divided into two regions: axial and appendicular (Figure A.10). The axial skeleton consists of the skull, vertebral column, and the thoracic cage formed by the ribs and sternum (breastbone). The appendicular skeleton comprises the pectoral girdle, the pelvic girdle, and all the bones of the upper and lower limbs.1
The Skull
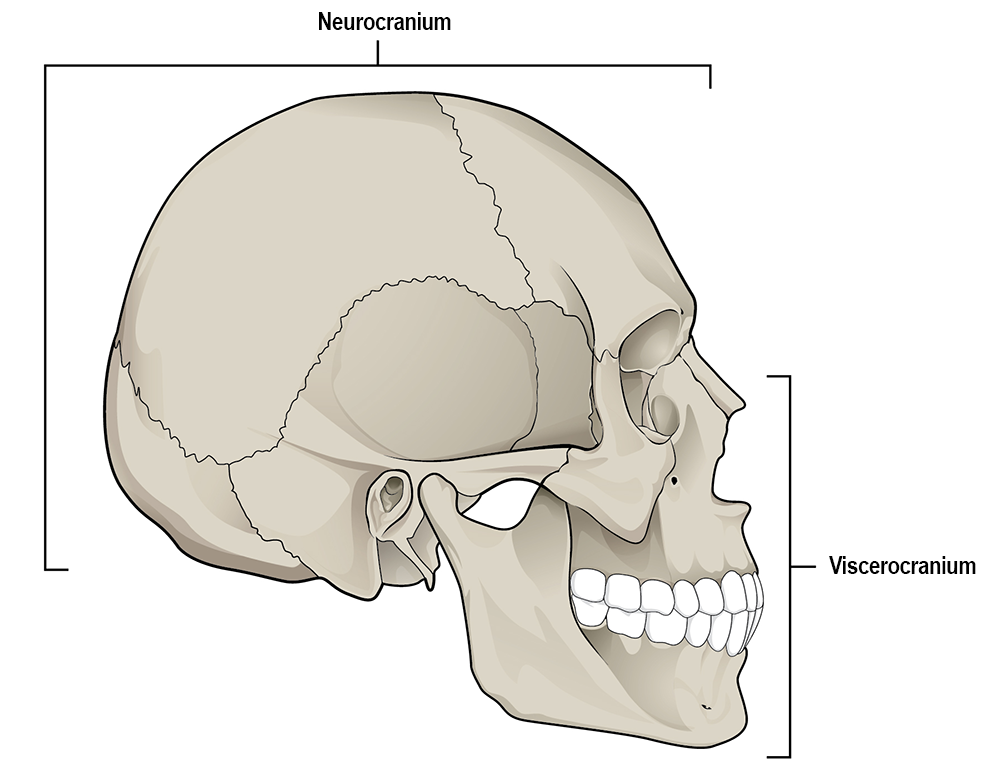
The cranium (skull) is the skeletal structure of the head that supports the face and protects the brain. It is subdivided into the facial bones and the brain case, or cranial vault (Figure A.11). The facial bones underlie the facial structures, form the nasal cavity, enclose the eyeballs, and support the teeth of the upper and lower jaws. The rounded brain case surrounds and protects the brain and houses the middle and inner ear structures.2
In the adult, the skull consists of 22 individual bones, 21 of which are immobile and united into a single unit. The 22nd bone is the mandible (lower jaw), which is the only moveable bone of the skull. ² The cranium is further subdivided into the neurocranium (or cranial vault), which houses the brain, and the viscerocranium (or facial skeleton; Figure A.11).1
Anterior View of Skull
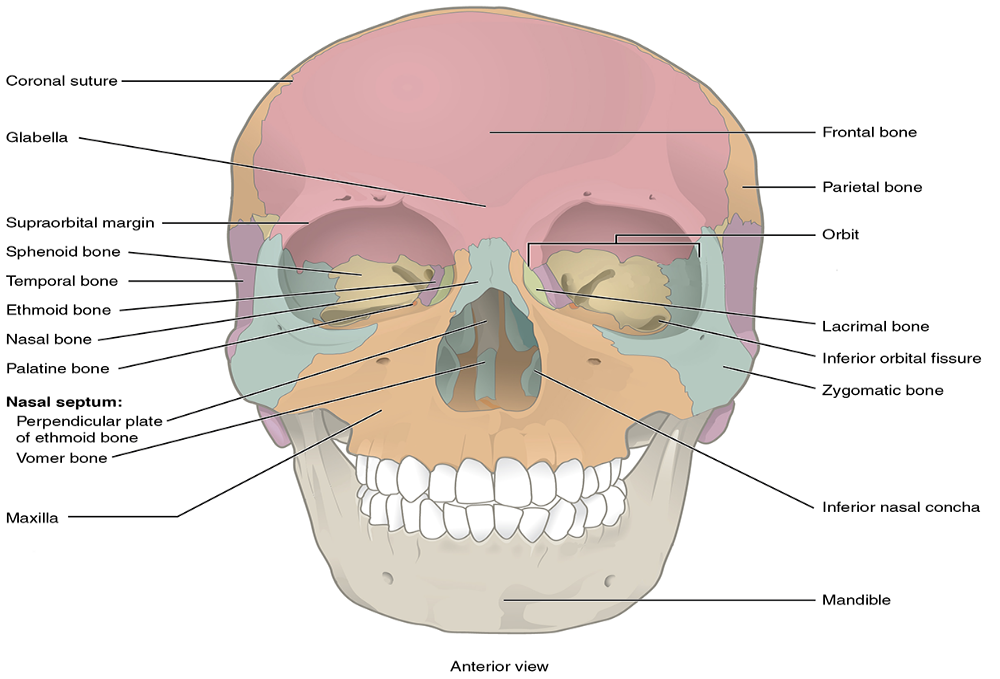
The anterior skull consists of the facial bones and provides the bony support for the eyes and structures of the face. This view of the skull is dominated by the openings of the orbits and the nasal cavity. Also seen are the upper and lower jaws, with their respective teeth.2
The orbit is the bony socket that houses the eyeball and muscles that move the eyeball or open the upper eyelid. The upper margin of the anterior orbit is the supraorbital margin. Located near the midpoint of the supraorbital margin is a small opening called the supraorbital foramen. This provides for passage of a sensory nerve to the skin of the forehead. Below the orbit is the infraorbital foramen, which is the point of emergence for a sensory nerve that supplies the anterior face below the orbit.2
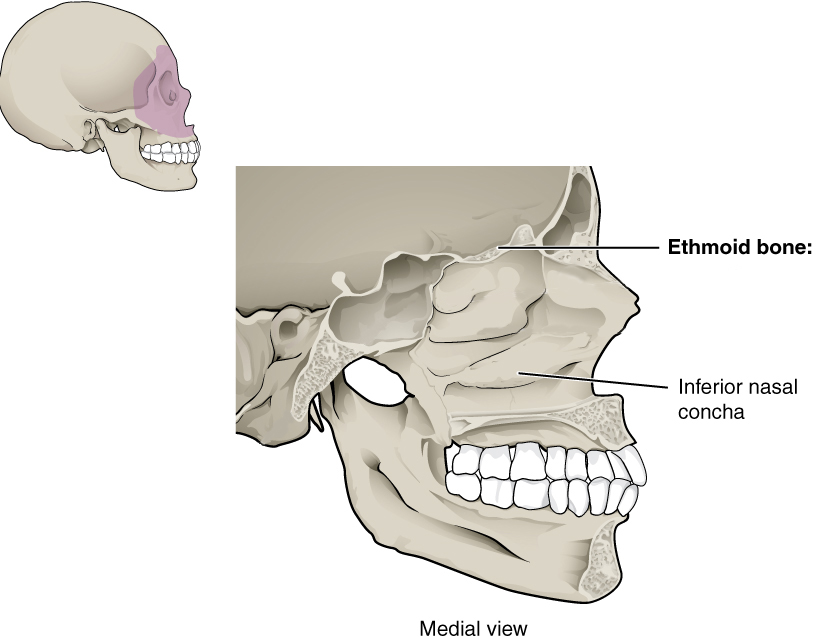
Inside the nasal area of the skull, the nasal cavity is divided into halves by the nasal septum. The upper portion of the nasal septum is formed by the perpendicular plate of the ethmoid bone and the lower portion is the vomer bone. Each side of the nasal cavity is triangular in shape, with a broad inferior space that narrows superiorly. When looking into the nasal cavity from the front of the skull, two bony plates are seen projecting from each lateral wall. The larger of these is the inferior nasal concha, an independent bone of the skull. Located just above the inferior concha is the middle nasal concha, which is part of the ethmoid bone. A third bony plate, also part of the ethmoid bone, is the superior nasal concha. It is much smaller and out of sight, above the middle concha. The superior nasal concha is located just lateral to the perpendicular plate, in the upper nasal cavity.2
Lateral View of Skull
A view of the lateral skull is dominated by the large, rounded brain case above and the upper and lower jaws with their teeth below. Separating these areas is the bridge of bone called the zygomatic arch. The zygomatic arch is the bony arch on the side of skull that spans from the area of the cheek to just above the ear canal. It is formed by the junction of two bony processes: a short anterior component, the temporal process of the zygomatic bone (the cheekbone) and a longer posterior portion, the zygomatic process of the temporal bone, extending forward from the temporal bone. Thus the temporal process (anteriorly) and the zygomatic process (posteriorly) join together, like the two ends of a drawbridge, to form the zygomatic arch. One of the major muscles that pulls the mandible upward during biting and chewing arises from the zygomatic arch.2
On the lateral side of the brain case, above the level of the zygomatic arch, is a shallow space called the temporal fossa. Below the level of the zygomatic arch and deep to the vertical portion of the mandible is another space called the infratemporal fossa. Both the temporal fossa and infratemporal fossa contain muscles that act on the mandible during chewing.2
Bones and Some Features of the Neurocranium
Frontal: an unpaired bone consisting of two parts: a superior, vertically oriented portion called the squama and an inferior, horizontally oriented portion that forms the roof of the orbit (eye socket; Figures A.12 and A.13).1
The coronal suture is the articulation between the frontal bone and the two parietal bones posterior and lateral to the frontal.
The frontal bone develops initially as two separate bones that fuse together during growth. Occasionally this fusion is incomplete, resulting in a metopic suture that persists between the two halves (left and right) of the frontal bone.1
The glabella is a bony projection between the brow ridges. The glabella in females tends to be flat while rounded and protruding in males.1
The supraorbital margin is the upper edge of the orbit. The thickness of the edge can be used as an indicator of sex. A thin, sharp border is indicative of a female while a blunt, thick border suggests a male.1
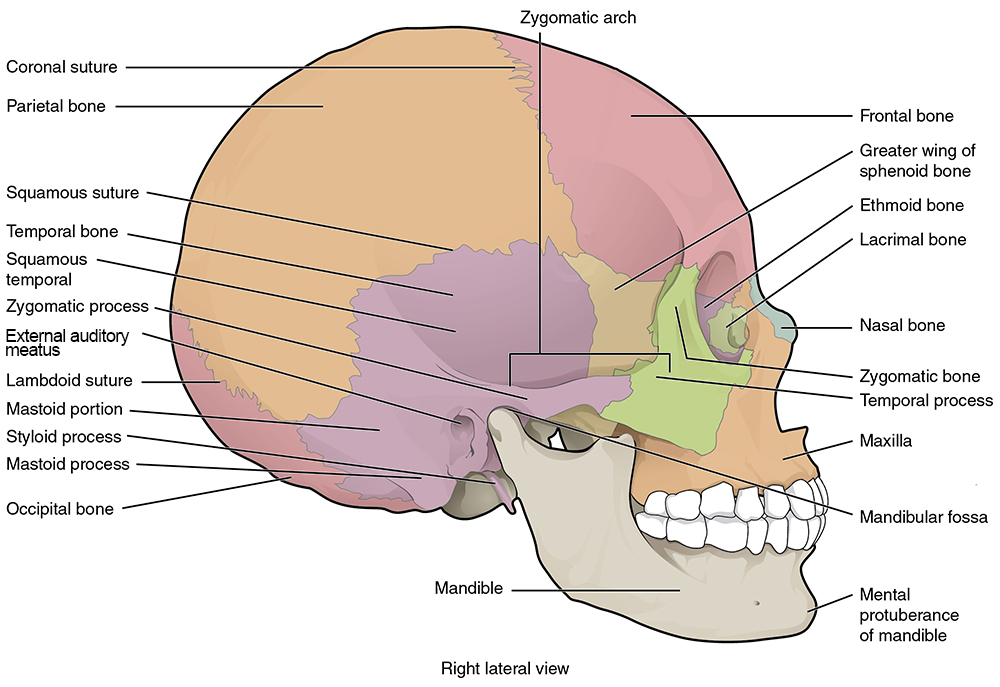
Parietal: Paired bones that form the majority of the roof and sides of the neurocranium (Figures A.12 and A.13).1 The sagittal suture is the articulation between the right and left parietal bones. It extends from the coronal suture anteriorly to the lambdoidal suture, which separates the parietal bones from the occipital bone posteriorly.1
Each parietal bone is marked by two temporal lines (superior and inferior), which are anterior-posterior arching lines that serve as attachment sites for a major chewing muscle (temporalis) and its associated connective tissue.1
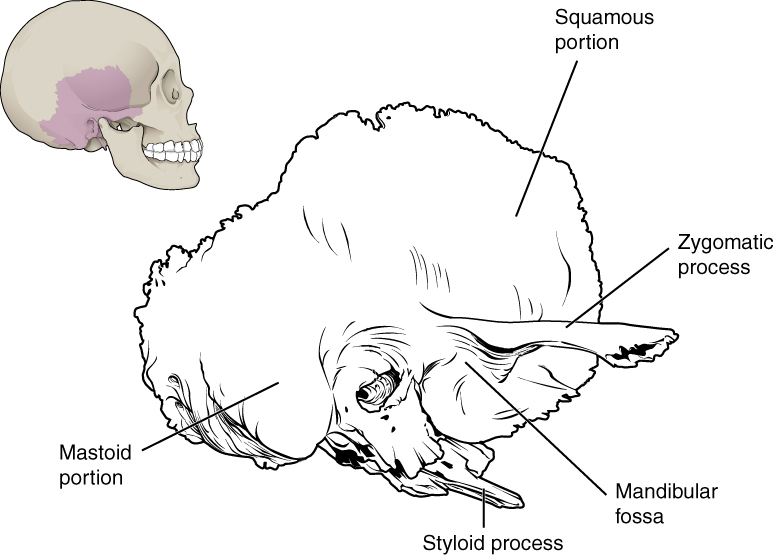
Temporal: Paired bones on the lateral side of the neurocranium that are divided into two portions: squamous (or flat) portion that forms the lateral side of the neurocranium and the petrous (or rock-like) portion that houses the special sense organs of the ear for hearing and balance as well as the three tiny bones of the middle ear: incus, malleus, and stapes (Figures A.13, A.14, and A.15).1
The squamosal suture is the articulation between the squamous portion of the temporal bone and the inferior border of the parietal bone.1
The mastoid process is a prominent attachment site for several muscles including the large sternocleidomastoid muscle. As such, it is often used to estimate sex in that males tend to have longer and wider mastoid processes compared to females (Bass 2005).1
The styloid process is a thin, pointed, inferior projection of the temporal bone that serves as an attachment site for several muscles and a ligament of the throat.1
The zygomatic process of the temporal is a thin, arch-like process that originates from the squamous portion of the temporal bone. The zygomatic process articulates with the temporal process of the zygomatic bone to form the zygomatic arch (or cheekbone).1
The temporal fossa is the depression in the temporal bone where the mandibular condyle (see below, under mandible) articulates to form the temporomandibular (or jaw) joint.1
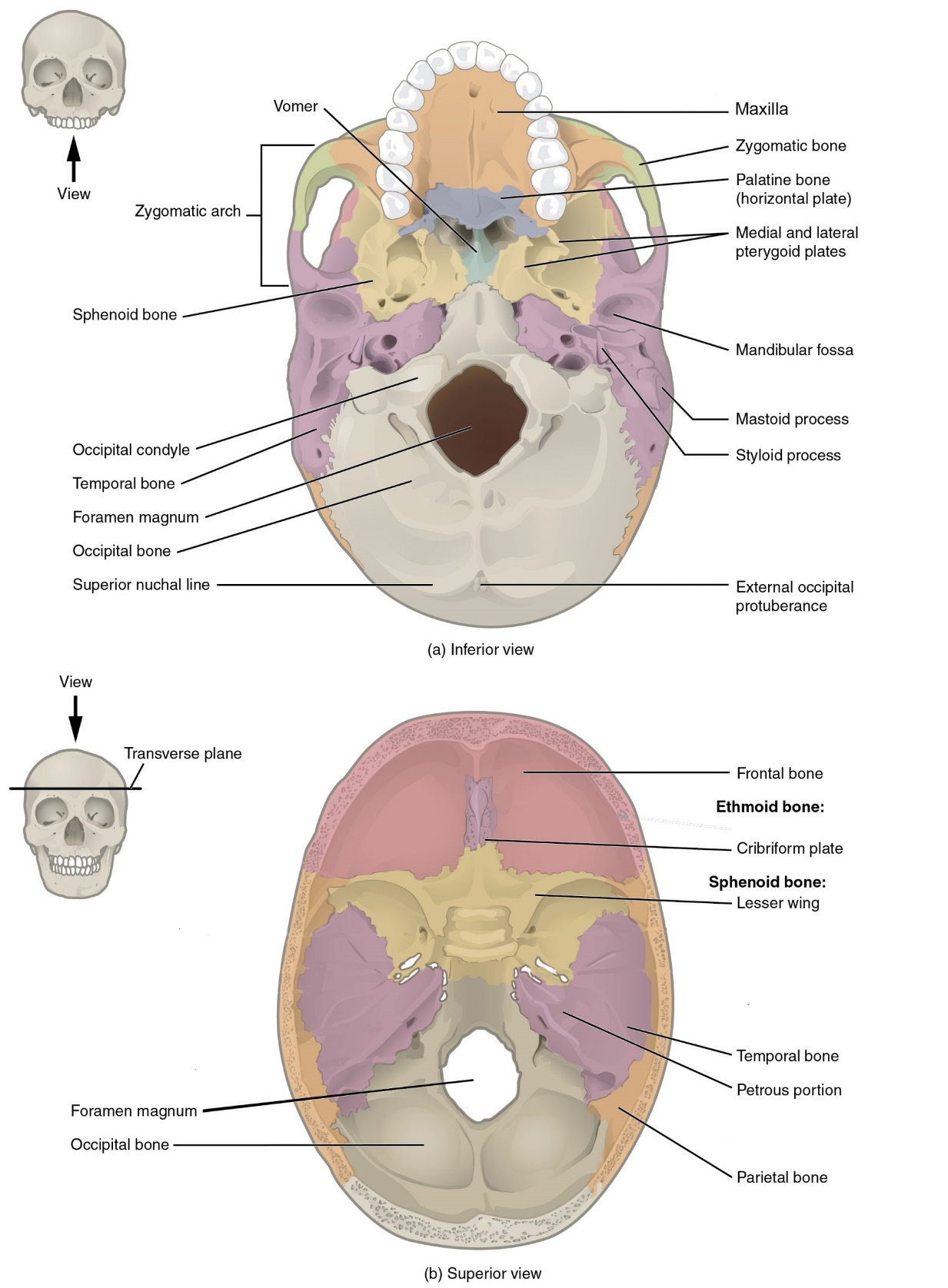
Occipital: Unpaired bone that forms the posterior and inferior portions of the neurocranium (Figures A.13 and A.15).1
The lambdoidal suture is the articulation between the occipital bone and the two parietal bones. It resembles the shape of the Greek letter lambda.1
The external occipital protuberance (EOP) is a robust attachment of the nuchal ligament. When viewed laterally, males tend to have a discernible projection or hook, whereas in females, the occipital is typically smooth.1
The nuchal lines are parallel ridges that meet on the midline at the EOP. These prominent muscle attachment sites tend to be more robust and projecting in males.1
The occipital bone contains a large circular opening called the foramen magnum, which provides a space for passage of the brainstem/spinal cord from the neurocranium into the vertebral canal of the spine.1
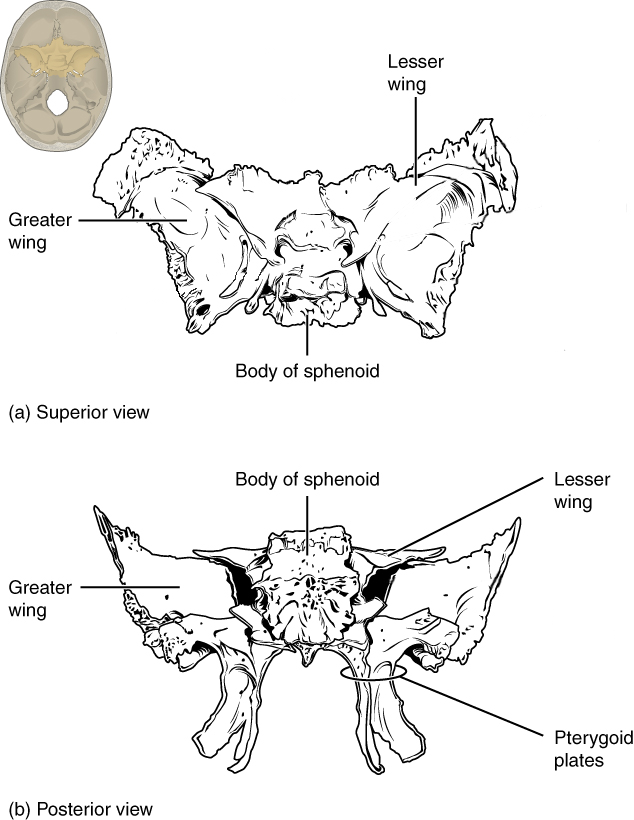
Sphenoid: Unpaired, butterfly-shaped bone that forms the central portion of the bottom of the neurocranium. The sphenoid is divided into several regions, including the body, greater wings, lesser wings, and pterygoid processes (with pterygoid plates; see Figures A.15 and A.16). This bone is critical to supporting the brain and several nerves and blood vessels supplying this region.1
Pterygoid plates are flat projections of the pterygoid processes that serve as attachment sites for chewing muscles and muscles of the throat.1
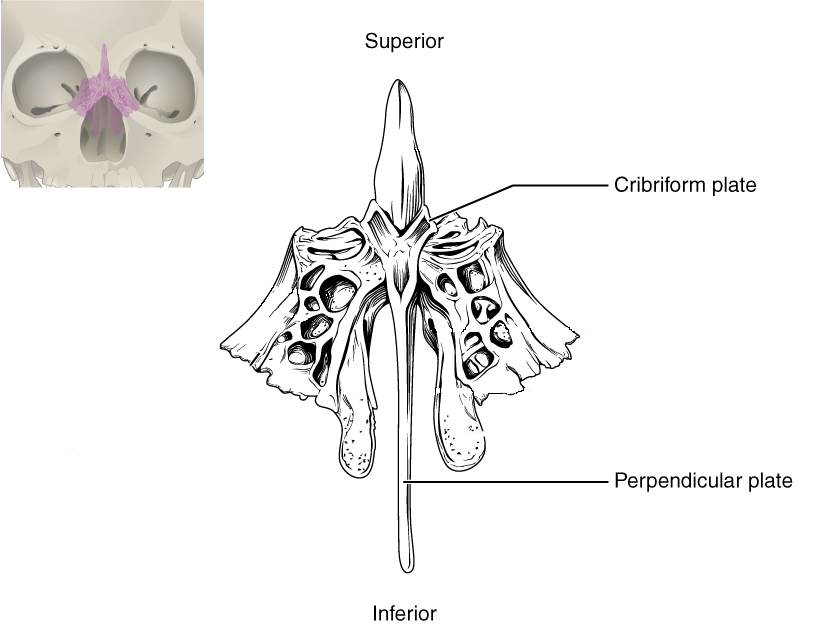
Ethmoid: Unpaired bone consisting of a median vertical plate that forms part of the bony nasal septum and a horizontal plate (cribriform plate) with many small foramina (holes) that transmit olfactory nerves (special sense of smell; Figure A.17).1
Bones of the Viscerocranium
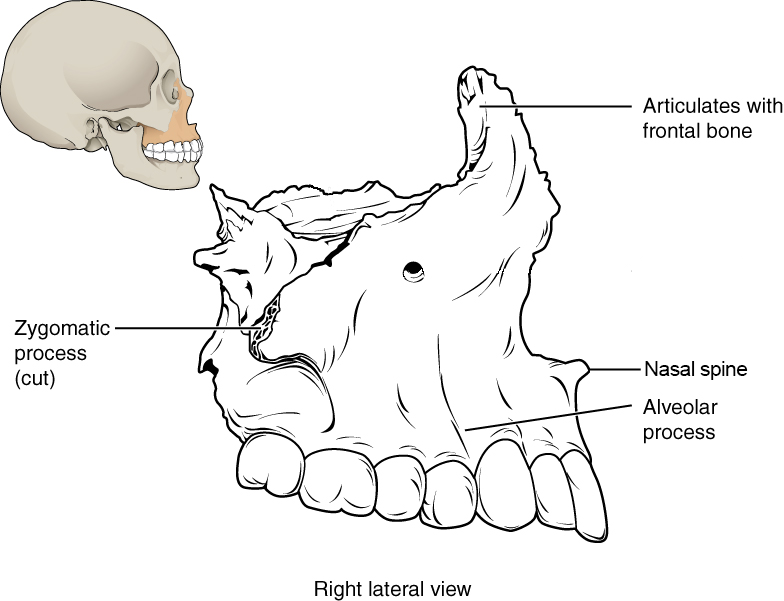
Maxilla: Paired bones that form the upper jaw, support the upper teeth, and form the inferior margin of the cheek (Figures A.12, A.13, A.15, and A.18).¹
The nasal spine is a thin projection on the midline at the inferior border of the nasal aperture. Length of the nasal spine has been used as a subjective trait to determine ancestry, with those exhibiting long nasal spines to be more likely of European ancestry.¹
The zygomatic process of the maxilla is the portion of the bone that articulates with the zygomatic bone to form the anterior portion of the zygomatic arch.¹
Nasal: Small, paired, flat, rectangular bones that form the bridge of the nose (Figure A.19).1
Nasal aperture is the anterior opening into the nasal cavity. As a forensic trait, it is described as low and wide in those of African ancestry and tall and narrow in those of European ancestry.1
Zygomatic: Paired bones that form the anterolateral portion of the cheekbone and contribute to the lateral and inferior wall of the orbit (Figure A.19).1
The temporal process of the zygomatic is the portion of the bone that articulates with the temporal bone to form the anterior portion of the zygomatic arch.1
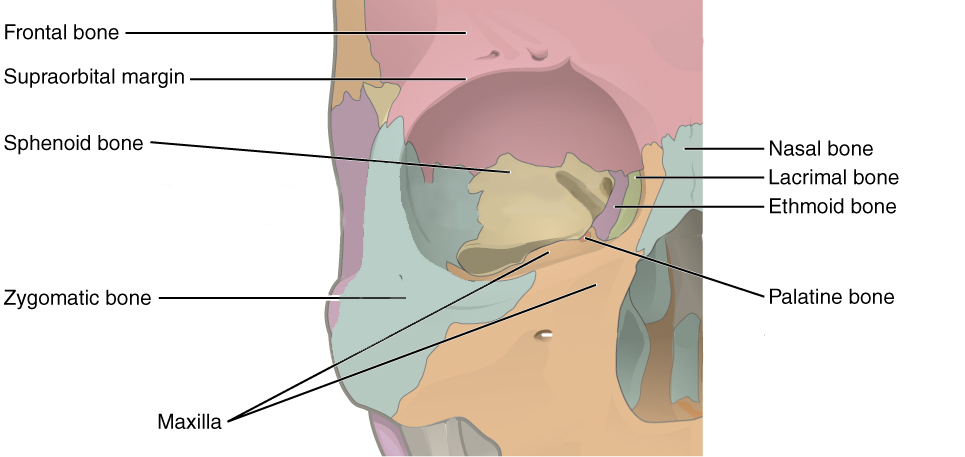
Palatine: Paired L-shaped bones that form the posterior portion of the roof of the mouth, floor of the orbit, and the floor and lateral walls of the nasal cavity (Figures A.15 and A.19).1
Lacrimal: Small, flat, paired bones that form the anterior portion of the medial wall of the orbit (Figure A.19).1
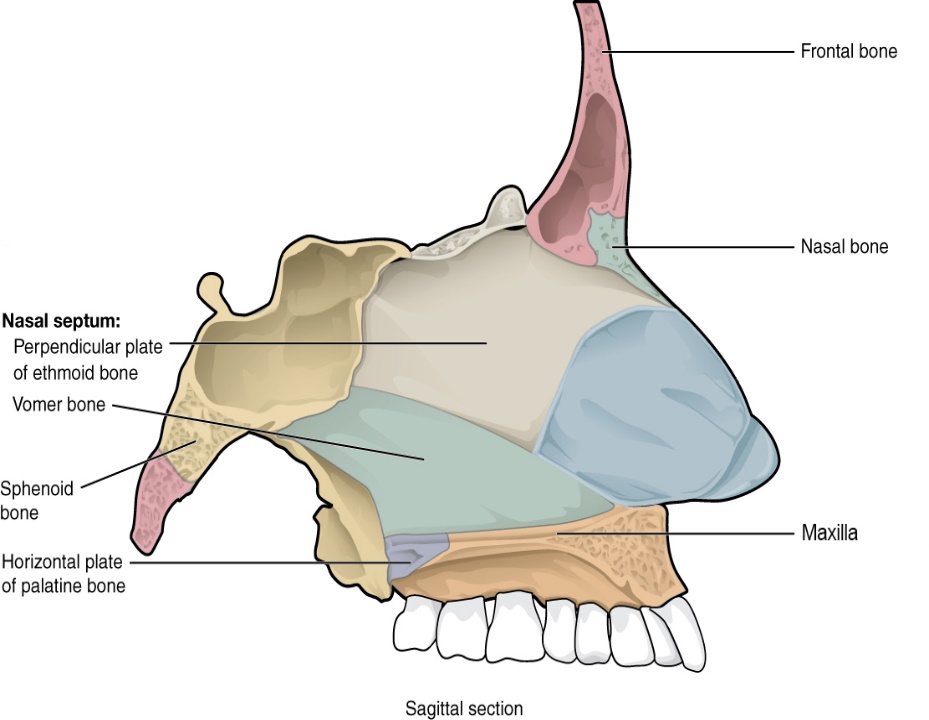
Vomer: Unpaired thin bone that forms the inferior portion of the bony nasal septum. It articulates with the ethmoid superiorly (Figure A.20).1
Inferior nasal concha: Paired bones that project and curl like a scroll from the lateral wall of the nasal cavity (Figure A.21).1
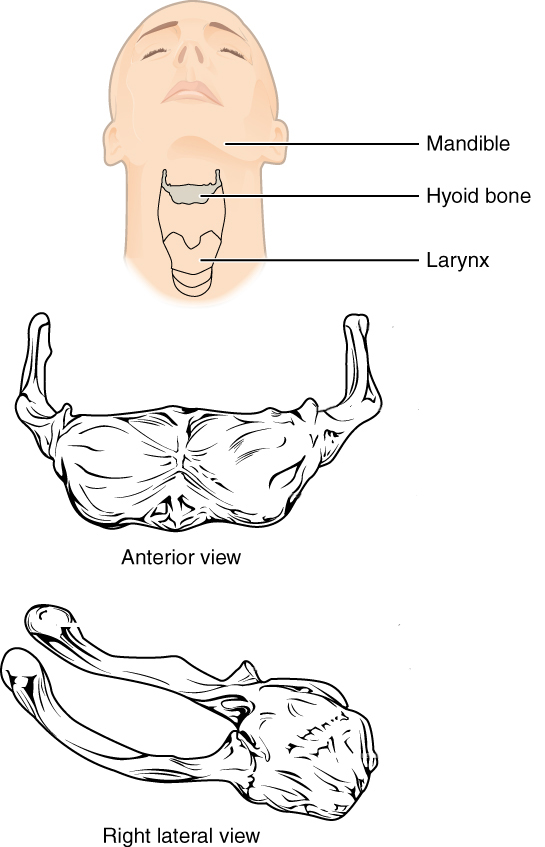
Hyoid: Unpaired U-shaped bone that sits in the neck inferior to the mandible. The hyoid is the only bone of the skeleton that does not articulate with another bone. Instead, it is encased in a sling of muscles that move the larynx (voice box), pharynx, and tongue (Figure A.22).1
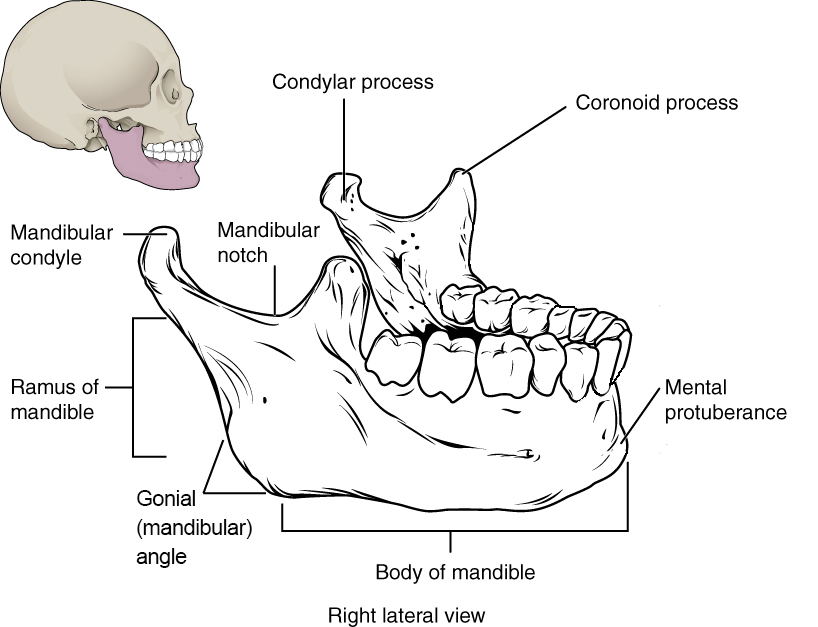
Mandible: Unpaired bone with a horizontal (and anteriorly arched) body and a vertical ramus that articulates with the temporal fossa to form the temporomandibular (jaw) joint. The body of the mandible houses the lower teeth (Figure A.13 and A.23).1
The mental protuberance (eminence) is the most anteriorly projecting point on the mandible—the so-called “chin.” A prominent projection is likely to indicate a male, while a smooth mental region likely indicates a female.1
The ramus of the mandible projects superiorly from the body of the mandible and ascends to one of two features on the superior aspect: coronoid process or mandibular condyle.1
The coronoid process is a bony projection off the anterior and superior aspect of the mandibular ramus. The inferior attachment of the temporalis muscle (a chewing muscle) attaches here.1
The mandibular condyle, a rounded projection off the posterior and superior aspect of the mandibular ramus, articulates with the temporal fossa of the temporal bone at the temporomandibular (TMJ) joint.1
The gonial (mandibular) angle is the rounded posteroinferior border of the mandible. It tends to be smooth in females with a more obtuse angle but is laterally flared in males and closer to a right angle in shape.1
Teeth: Adults normally have 32 teeth, distributed among four quadrants of the mouth (upper left, upper right, lower left, lower right). In each quadrant, there are eight teeth: two incisors (central and lateral), one canine, two premolars, and three molars. Each of these types of teeth has a different shape that reflects its function during chewing:
Incisors are flat and shovel-shaped and are used to bite into a food item.
Canines are conical, with a single pointed cusp used to puncture a food item.
Premolars have two rounded cusps and are used to grind and mash a food item.
Molars have five flatter cusps and are used to grind food prior to swallowing.1
The Vertebral Column
The vertebral column is also known as the spinal column or spine. It consists of a sequence of vertebrae (singular = vertebra), each of which is separated and united by an intervertebral disc. Together, the vertebrae and intervertebral discs form the vertebral column. It is a flexible column that supports the head, neck, and body and allows for their movements. It also protects the spinal cord, which passes down the back through openings in the vertebrae.2
Regions of the Vertebral Column
The vertebral column originally develops as a series of 33 vertebrae, but this number is eventually reduced to 24 vertebrae, plus the sacrum and coccyx. The vertebral column is subdivided into five regions, with the vertebrae in each area named for that region and numbered in descending order. In the neck, there are seven cervical vertebrae, each designated with the letter “C” followed by its number. Superiorly, the C1 vertebra articulates (forms a joint) with the occipital condyles of the skull. Inferiorly, C1 articulates with the C2 vertebra, and so on. Below these are the 12 thoracic vertebrae, designated T1–T12. The lower back contains the L1–L5 lumbar vertebrae. The single sacrum, which is also part of the pelvis, is formed by the fusion of five sacral vertebrae. Similarly, the coccyx, or tailbone, results from the fusion of four small coccygeal vertebrae.2
An interesting anatomical fact is that almost all mammals have seven cervical vertebrae, regardless of body size. This means that there are large variations in the size of cervical vertebrae, ranging from the very small cervical vertebrae of a shrew to the greatly elongated vertebrae in the neck of a giraffe. In a full-grown giraffe, each cervical vertebra is 11 inches tall.2
General Structure of a Vertebra
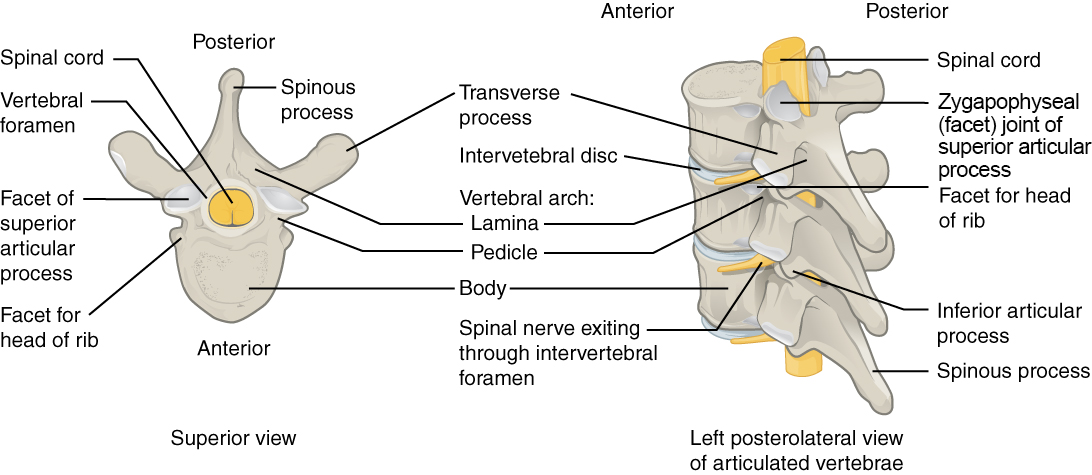
Within the different regions of the vertebral column, vertebrae vary in size and shape, but they all follow a similar structural pattern.2 A typical vertebra consists of an anteriorly situated body—the main weight-bearing element of the vertebra—and a posteriorly projecting vertebral arch (Figure A.24). The vertebral arch consists of the paired pedicles and paired laminae. The pedicle connects the transverse process (a laterally projecting process that serves as an attachment site for muscles and ligaments) to the vertebral body; the lamina connects the spinous process (a posteriorly projecting process that serves as an attachment site for muscles and ligaments) to the transverse process. Projecting inferiorly off the vertebral arch is the inferior articular process, and projecting superiorly off the vertebral arch is the superior articular process. Between the vertebral body anteriorly and the vertebral arch posteriorly is an open space called the vertebral foramen.1
Adjacent vertebrae articulate with one another through two major types of joints: intervertebral disc joints between adjacent vertebral bodies and zygapophyseal (facet) joints between the inferior articular process of one vertebra and the superior articular process of the vertebra immediately inferior to it. When all vertebrae are articulated into a column, the adjacent vertebral foramina form the vertebral canal, through which the spinal cord travels from the foramen magnum of the occipital bone to approximately the level of the second lumbar vertebra. At the level of each vertebra, the spinal cord gives us a pair (left and right) of spinal nerves that exit between adjacent vertebrae through the intervertebral foramen formed by adjacent vertebral arches. Even though the spinal cord ends in the lumbar region, the spinal nerves emanating from the spinal cord continue all the way to the sacrum (sometimes to the coccyx), culminating in a total of 30–31 pairs of spinal nerves.1
Regional Differences in Vertebral Shape
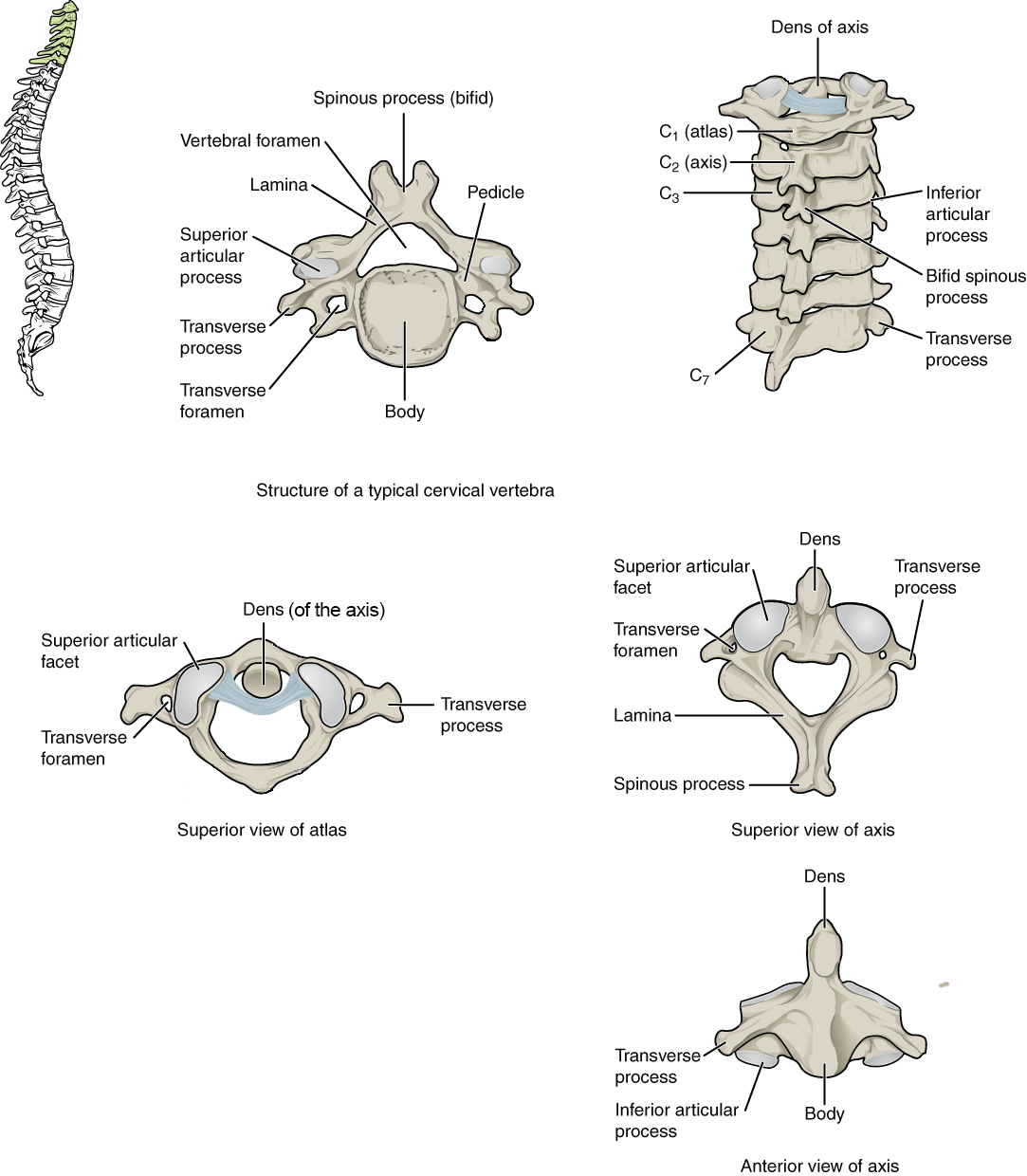
In the cervical region of the vertebral column, there are seven vertebrae (named C1–C7 from superior to inferior; Figure A.25). The first two cervical vertebrae are unique from each other and all other cervical vertebrae, and they get special names: atlas (C1) and axis (C2). The atlas lacks a vertebral body (having only two large articular facets for articulation with the occipital bone of the skull: the atlanto-occipital joint for nodding the head) and does not have a spinous process. The axis is notable for the superiorly projecting dens (or odontoid process), which articulates with the atlas to create the atlanto-axial joint for head rotation. Otherwise, a typical cervical vertebra has a small vertebral body, a bifid (split) spinous process, a transverse process with a transverse foramen on it for passage of the vertebral artery and vein, and a triangular-shaped vertebral foramen.1
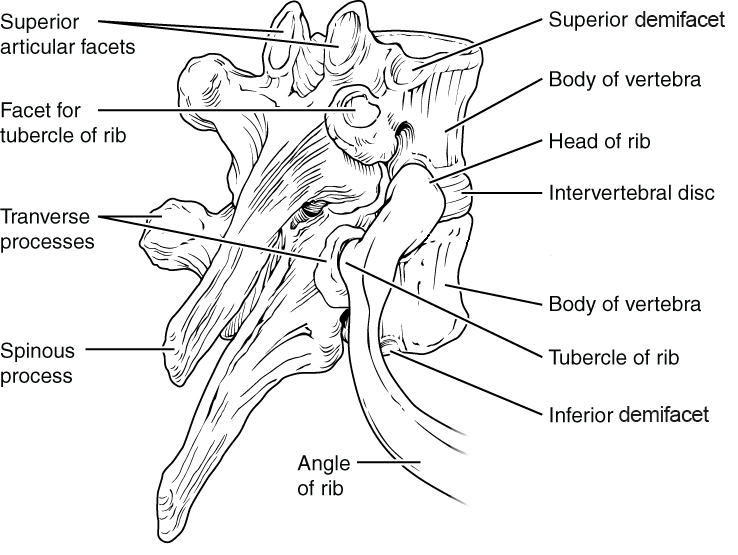
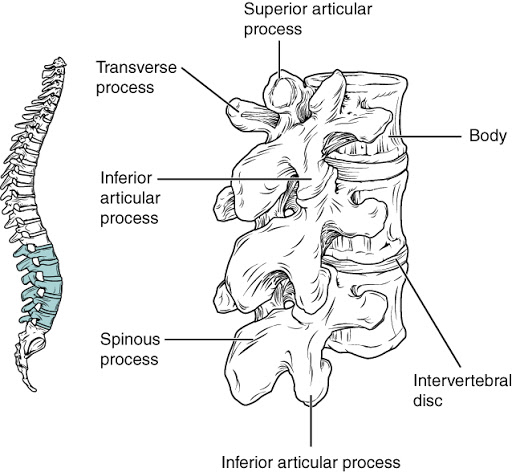
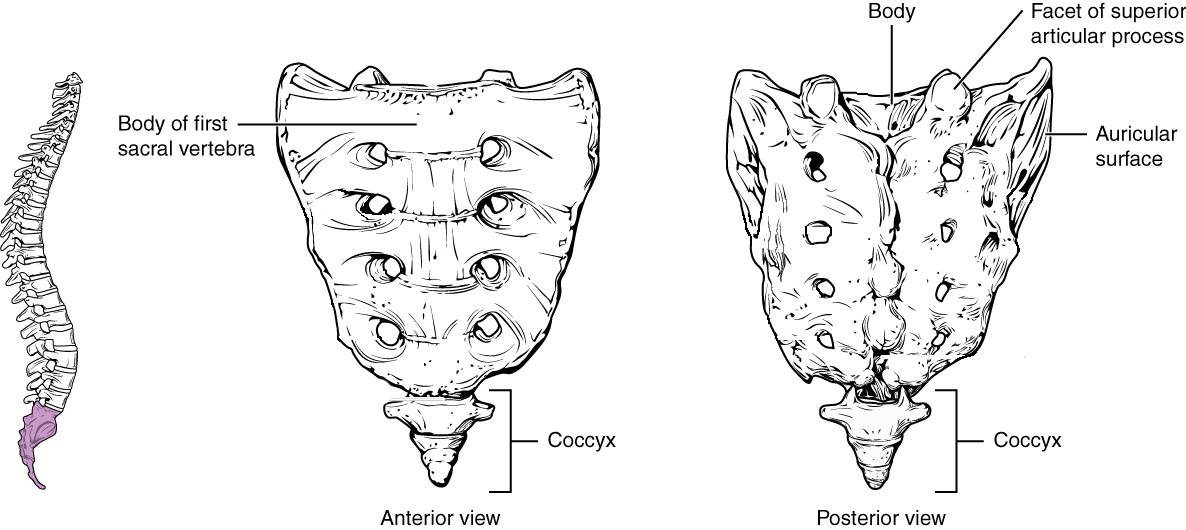
The vertebrae in the other regions of the spinal column are less variable in shape than the cervical region vertebrae. There are 12 thoracic region vertebrae (T1–T12), and they can be easily distinguished from the vertebrae in other regions because they have articular facets on their vertebral bodies for articulation with the head of a rib, as well as articular facets on the transverse process for articulation with the rib tubercle (Figure A.26). In particular, the vertebral bodies of T2–T9 have two pairs of articular facets called demifacets (superior and inferior), for articulation with multiple ribs; T1 and T10–T12 have single facets for articulation with a single rib. All five lumbar region vertebrae (L1–L5) are distinguished by their large vertebral body and rounded spinous process (Figure A.27). Finally, there is the sacrum, which is a bone of the pelvis that forms from the fusion of all five sacral region vertebrae (S1–S5), and there is the coccyx, which comprises three to four fused coccygeal region vertebrae that form the tailbone (Figure A.28). All great apes (including humans) lack an external tail; the coccygeal vertebrae are homologs of the external tail vertebrae in other primates and mammals (Organ 2017). Homologs are anatomical features that have the same evolutionary origin but do not necessarily have identical structure or function (i.e., the wings of bats and the arms of humans are homologous).1
Curvatures of the Vertebral Column
The adult vertebral column does not form a straight line, but instead has four curvatures along its length (see Figure A.28). These curves increase the vertebral column’s strength, flexibility, and ability to absorb shock. When the load on the spine is increased, by carrying a heavy backpack for example, the curvatures increase in depth (become more curved) to accommodate the extra weight. They then spring back when the weight is removed. The four adult curvatures are classified as either primary or secondary curvatures. Primary curves are retained from the original fetal curvature, while secondary curvatures develop after birth.2
During fetal development, the body is flexed anteriorly into the fetal position, giving the entire vertebral column a single curvature that is concave anteriorly. In the adult, this fetal curvature is retained in two regions of the vertebral column as the thoracic curve, which involves the thoracic vertebrae, and the sacrococcygeal curve, formed by the sacrum and coccyx. Each of these is thus called a primary curve because they are retained from the original fetal curvature of the vertebral column.2
A secondary curve develops gradually after birth as the child learns to sit upright, stand, and walk. Secondary curves are concave posteriorly, opposite in direction to the original fetal curvature. The cervical curve of the neck region develops as the infant begins to hold their head upright when sitting. Later, as the child begins to stand and then to walk, the lumbar curve of the lower back develops. In adults, the lumbar curve is generally deeper in females.2
Thoracic Cage
The thoracic cage is formed from the sternum and the 12 ribs and their cartilages (costal cartilages), and the 12 thoracic vertebrae with which the ribs articulate (Figure A.30).1
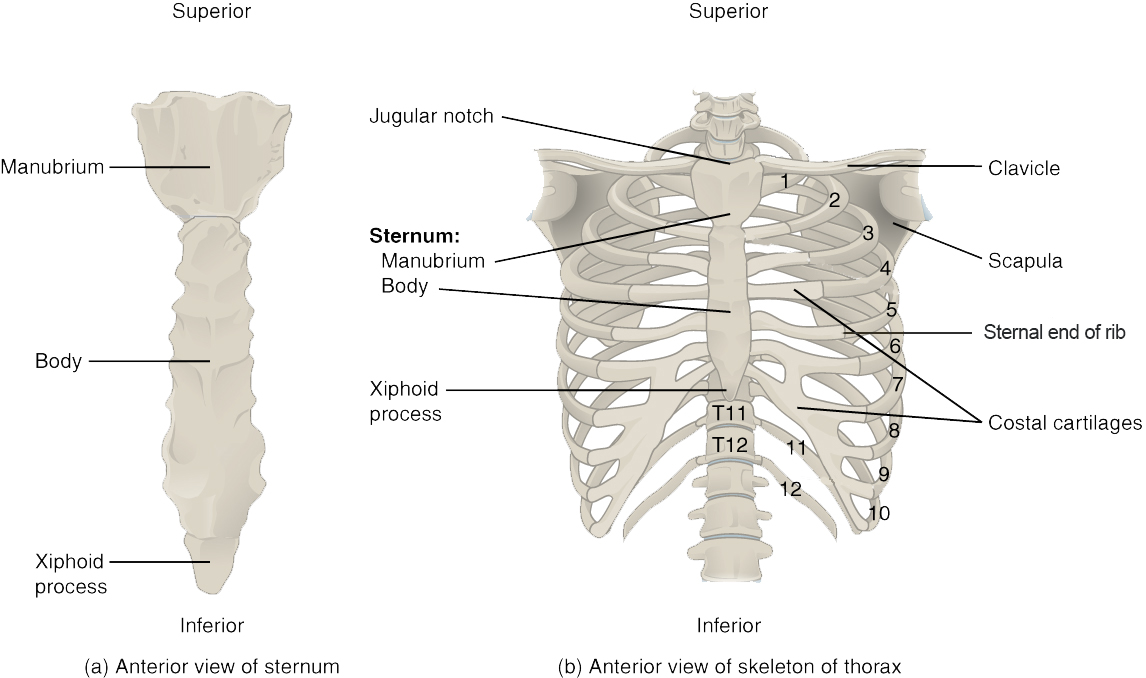
Sternum
The sternum is the elongated bony structure that anchors the anterior thoracic cage. It consists of three parts: the manubrium, body, and xiphoid process. The manubrium is the wider, superior portion of the sternum. The top of the manubrium has a shallow, U-shaped border called the jugular (suprasternal) notch. This can be easily felt at the anterior base of the neck, between the medial ends of the clavicles. The clavicular notch is the shallow depression located on either side at the superior-lateral margins of the manubrium. This is the site of the sternoclavicular joint, between the sternum and clavicle. The first ribs also attach to the manubrium.2
The elongated, central portion of the sternum is the body. The manubrium and body join together at the sternal angle, so called because the junction between these two components is not flat, but forms a slight bend. The second rib attaches to the sternum at the sternal angle. Since the first rib is hidden behind the clavicle, the second rib is the highest rib that can be identified by palpation. Thus, the sternal angle and second rib are important landmarks for the identification and counting of the lower ribs. Ribs 3–7 attach to the sternal body.2
The inferior tip of the sternum is the xiphoid process. This small structure is cartilaginous early in life, but gradually becomes ossified starting during middle age.2
Ribs
Each rib has a head and neck (with rib tubercle) at the vertebral end of the rib as well as a flattened shaft that extends to articulate with the sternum. All ribs articulate with the vertebral column at two points: the transverse process facet (rib tubercle) and vertebral body articular facet (head of rib). But articulations between the ribs and the sternum vary, where some ribs (1–7, the “true ribs”) attach directly to the sternum via their costal cartilages, other ribs (8–10, the “false ribs”) attach indirectly to the sternum via the costal cartilage of the rib above, and some ribs (11–12, the “floating ribs”) do not attach to the sternum at all. With increasing age, the sternal end of the rib becomes thinner and irregularly shaped compared to the smooth, rounded shape seen in young adults.1
Appendicular Skeleton
Pectoral Girdle
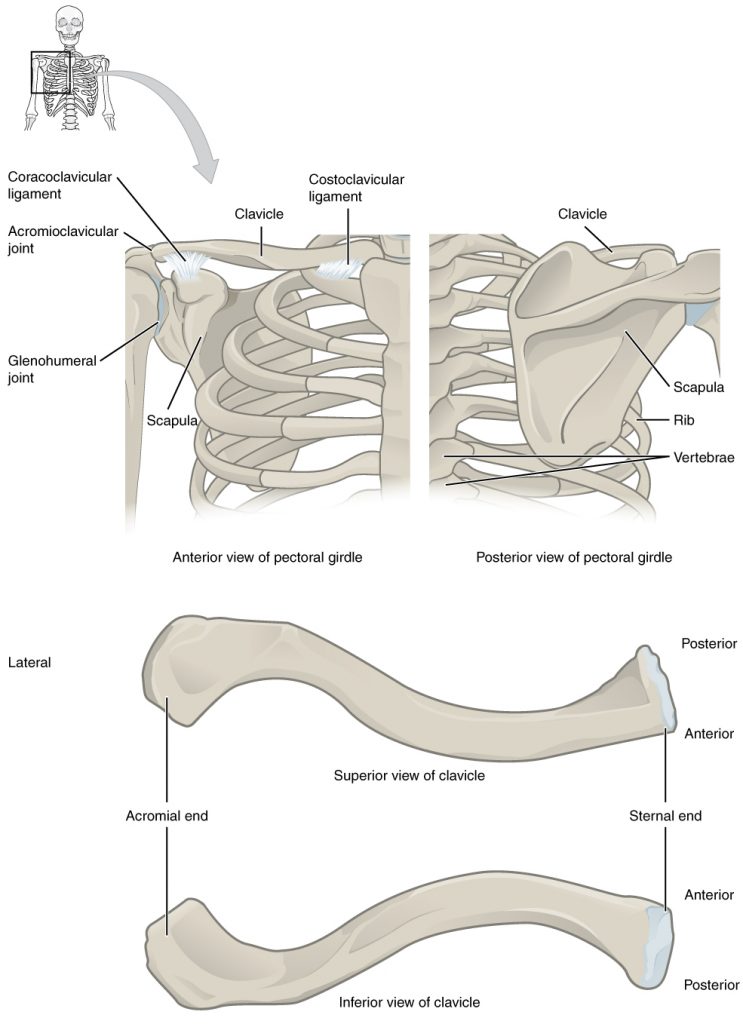
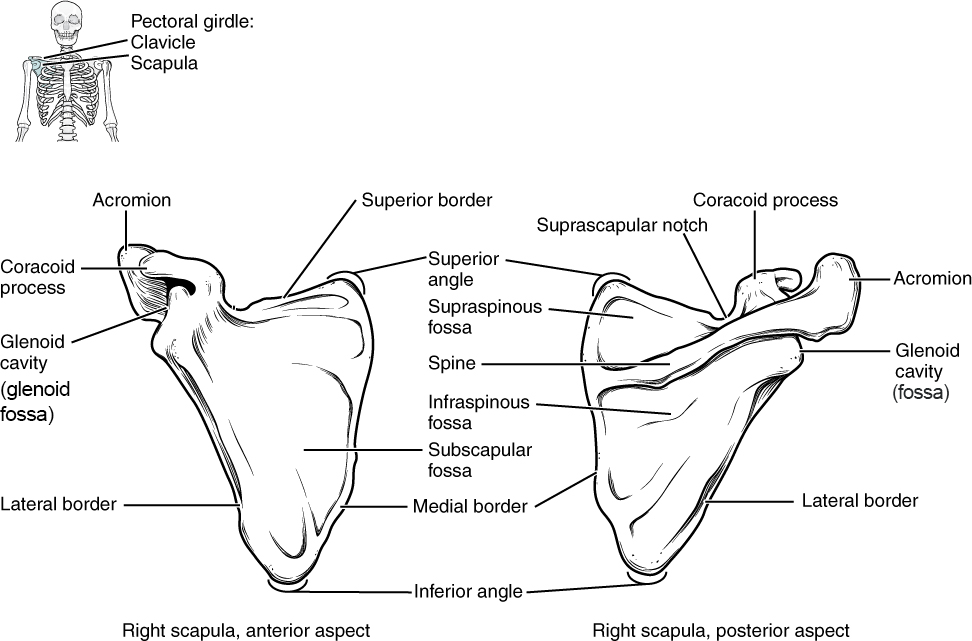
The pectoral girdle consists of the clavicle and the scapula, and it serves as the proximal base of the upper limb as well as the anchor for the upper limb to the axial skeleton. The clavicle is an S-shaped bone, and it forms the strut that connects the scapula to the sternum (Figure A.31). The scapula is a large, flat bone with three angles (superior, inferior, and lateral) and three borders (medial, lateral, and superior). The lateral angle is noteworthy because it serves as the articulation for the head of the humerus of the upper limb at the glenoid cavity (or glenoid fossa; Figure A.32). The borders and the anterior and posterior surfaces of the scapula are sites of muscle attachment. The scapula also has three important projections for muscle and ligament attachments: the coracoid process anteriorly and superiorly; the acromion, which articulates with the lateral end of the clavicle; and the spine on the posterior aspect of the scapula.1
Bones of the Upper Limb
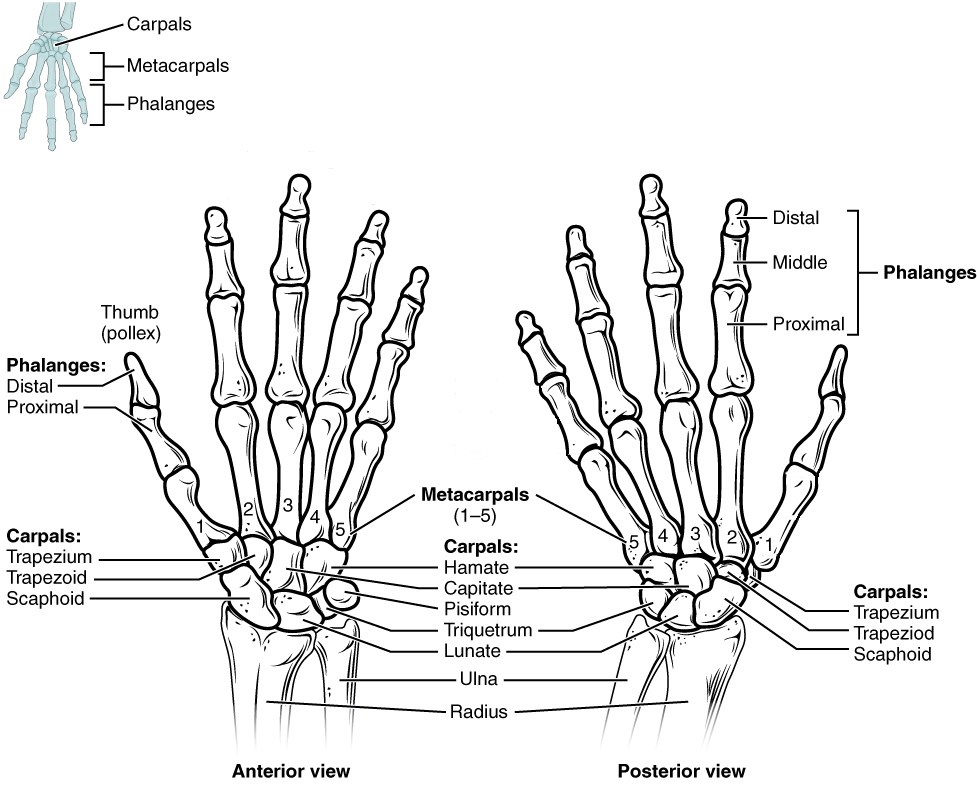
The upper limb is divided into three regions. These consist of the arm, located between the shoulder and elbow joints; the forearm, which is between the elbow and wrist joints; and the hand, which is located distal to the wrist. There are 30 bones in each upper limb (see Chapter 8.1 Figure 1). The humerus is the single bone of the upper arm, and the ulna (medially) and the radius (laterally) are the paired bones of the forearm. The base of the hand contains eight bones, each called a carpal bone, and the palm of the hand is formed by five bones, each called a metacarpal bone. The fingers and thumb contain a total of 14 bones, each of which is a phalanx bone of the hand.²
Humerus
The humerus is the single bone of the upper arm region (Figure A.33). At its proximal end is the head of the humerus. This is the large, round, smooth region that faces medially. The head articulates with the glenoid cavity of the scapula to form the glenohumeral (shoulder) joint. The margin of the smooth area of the head is the anatomical neck of the humerus. Located on the lateral side of the proximal humerus is an expanded bony area called the greater tubercle. The smaller lesser tubercle of the humerus is found on the anterior aspect of the humerus. Both the greater and lesser tubercles serve as attachment sites for muscles that act across the shoulder joint. Passing between the greater and lesser tubercles is the narrow intertubercular groove (sulcus), which is also known as the bicipital groove because it provides passage for a tendon of the biceps brachii muscle. The surgical neck is located at the base of the expanded, proximal end of the humerus, where it joins the narrow shaft of the humerus. The surgical neck is a common site of arm fractures. The deltoid tuberosity is a roughened, V-shaped region located on the lateral side in the middle of the humerus shaft. As its name indicates, it is the site of attachment for the deltoid muscle.2
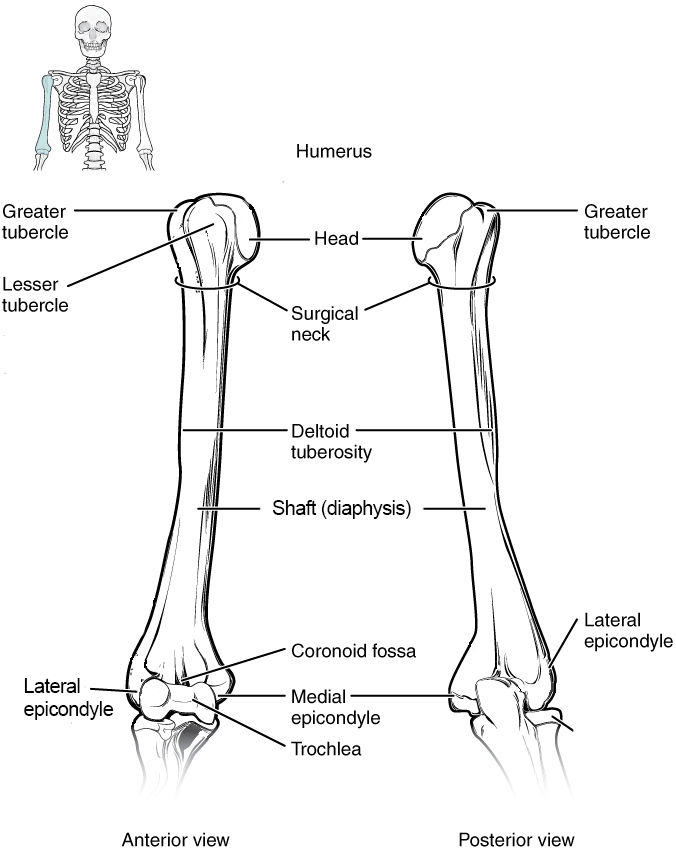
Distally, the humerus becomes flattened. The prominent bony projection on the medial side is the medial epicondyle of the humerus. The much smaller lateral epicondyle of the humerus is found on the lateral side of the distal humerus. The roughened ridge of bone above the lateral epicondyle is the lateral supracondylar ridge. All of these areas are attachment points for muscles that act on the forearm, wrist, and hand. The powerful grasping muscles of the anterior forearm arise from the medial epicondyle, which is thus larger and more robust than the lateral epicondyle that gives rise to the weaker posterior forearm muscles.2
The distal end of the humerus has two articulation areas, which join the ulna and radius bones of the forearm to form the elbow joint. The more medial of these areas is the trochlea, a spindle- or pulley-shaped region (trochlea = “pulley”), which articulates with the ulna bone. Immediately lateral to the trochlea is the capitulum (“small head”), a knob-like structure located on the anterior surface of the distal humerus. The capitulum articulates with the radius bone of the forearm. Just above these bony areas are two small depressions. These spaces accommodate the forearm bones when the elbow is fully bent (flexed). Superior to the trochlea is the coronoid fossa, which receives the coronoid process of the ulna, and above the capitulum is the radial fossa, which receives the head of the radius when the elbow is flexed. Similarly, the posterior humerus has the olecranon fossa, a larger depression that receives the olecranon process of the ulna when the forearm is fully extended.2
Ulna
The ulna is the medial bone of the forearm. It runs parallel to the radius, which is the lateral bone of the forearm (Figure A. 34). The proximal end of the ulna resembles a crescent wrench with its large, C-shaped trochlear notch. This region articulates with the trochlea of the humerus as part of the elbow joint. The inferior margin of the trochlear notch is formed by a prominent lip of bone called the coronoid process of the ulna. Just below this on the anterior ulna is a roughened area called the ulnar tuberosity. To the lateral side and slightly inferior to the trochlear notch is a small, smooth area called the radial notch of the ulna. This area is the site of articulation between the proximal radius and the ulna, forming the proximal radioulnar joint. The posterior and superior portions of the proximal ulna make up the olecranon process, which forms the bony tip of the elbow.2
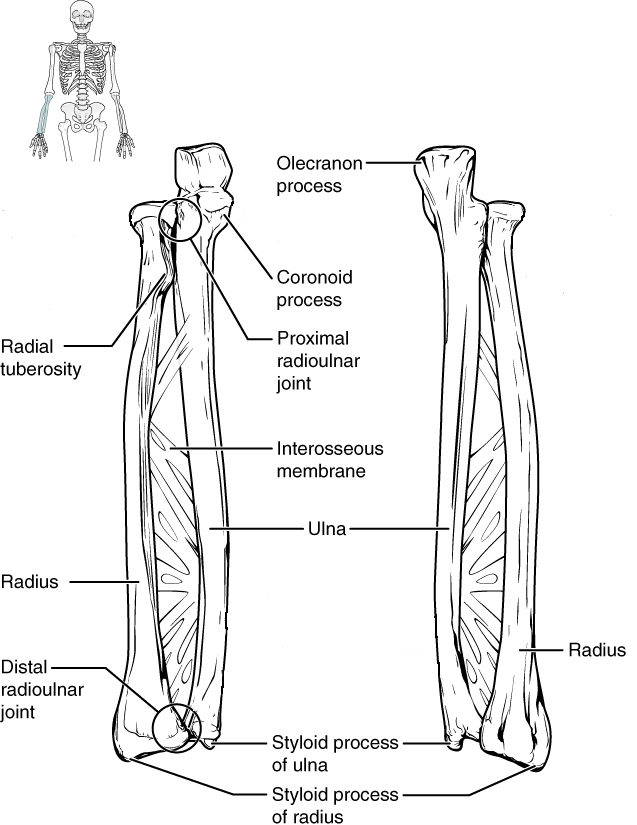
More distal is the shaft of the ulna. The lateral side of the shaft forms a ridge called the interosseous border of the ulna. This is the line of attachment for the interosseous membrane of the forearm, a sheet of dense connective tissue that unites the ulna and radius bones. The small, rounded area that forms the distal end is the head of the ulna. Projecting from the posterior side of the ulnar head is the styloid process of the ulna, a short bony projection. This serves as an attachment point for a connective tissue structure that unites the distal ends of the ulna and radius.2
In the anatomical position, with the elbow fully extended and the palms facing forward, the arm and forearm do not form a straight line. Instead, the forearm deviates laterally by 5–15 degrees from the line of the arm. This deviation is called the carrying angle. It allows the forearm and hand to swing freely or to carry an object without hitting the hip. The carrying angle is larger in females to accommodate their wider pelvis.2
Radius
The radius runs parallel to the ulna, on the lateral (thumb) side of the forearm (see Figure A.34). The head of the radius is a disc-shaped structure that forms the proximal end. The small depression on the surface of the head articulates with the capitulum of the humerus as part of the elbow joint, whereas the smooth, outer margin of the head articulates with the radial notch of the ulna at the proximal radioulnar joint. The neck of the radius is the narrowed region immediately below the expanded head. Inferior to this point on the medial side is the radial tuberosity, an oval-shaped, bony protuberance that serves as a muscle attachment point. The shaft of the radius is slightly curved and has a small ridge along its medial side. This ridge forms the interosseous border of the radius, which, like the similar border of the ulna, is the line of attachment for the interosseous membrane that unites the two forearm bones. The distal end of the radius has a smooth surface for articulation with two carpal bones to form the radiocarpal joint or wrist joint. On the medial side of the distal radius is the ulnar notch of the radius. This shallow depression articulates with the head of the ulna, which together form the distal radioulnar joint. The lateral end of the radius has a pointed projection called the styloid process of the radius. This provides attachment for ligaments that support the lateral side of the wrist joint. Compared to the styloid process of the ulna, the styloid process of the radius projects more distally, thereby limiting the range of movement for lateral deviations of the hand at the wrist joint.
Carpal Bones
The wrist and base of the hand are formed by a series of eight small carpal bones (see Figure A.35). The carpal bones are arranged in two rows, forming a proximal row of four carpal bones and a distal row of four carpal bones. The bones in the proximal row, running from the lateral (thumb) side to the medial side, are the scaphoid (“boat-shaped”), lunate (“moon-shaped”), triquetrum (“three-cornered”), and pisiform (“pea-shaped”) bones. The small, rounded pisiform bone articulates with the anterior surface of the triquetrum bone. The pisiform thus projects anteriorly, where it forms the bony bump that can be felt at the medial base of your hand. The distal bones (lateral to medial) are the trapezium (“table”), trapezoid (“resembles a table”), capitate (“head-shaped”), and hamate (“hooked bone”) bones. The hamate bone is characterized by a prominent bony extension on its anterior side called the hook of the hamate bone.2
A helpful mnemonic for remembering the arrangement of the carpal bones is “So Long To Pinky, Here Comes The Thumb.” This mnemonic starts on the lateral side and names the proximal bones from lateral to medial (scaphoid, lunate, triquetrum, pisiform), then makes a U-turn to name the distal bones from medial to lateral (hamate, capitate, trapezoid, trapezium). Thus, it starts and finishes on the lateral side.2
Pelvic Girdle
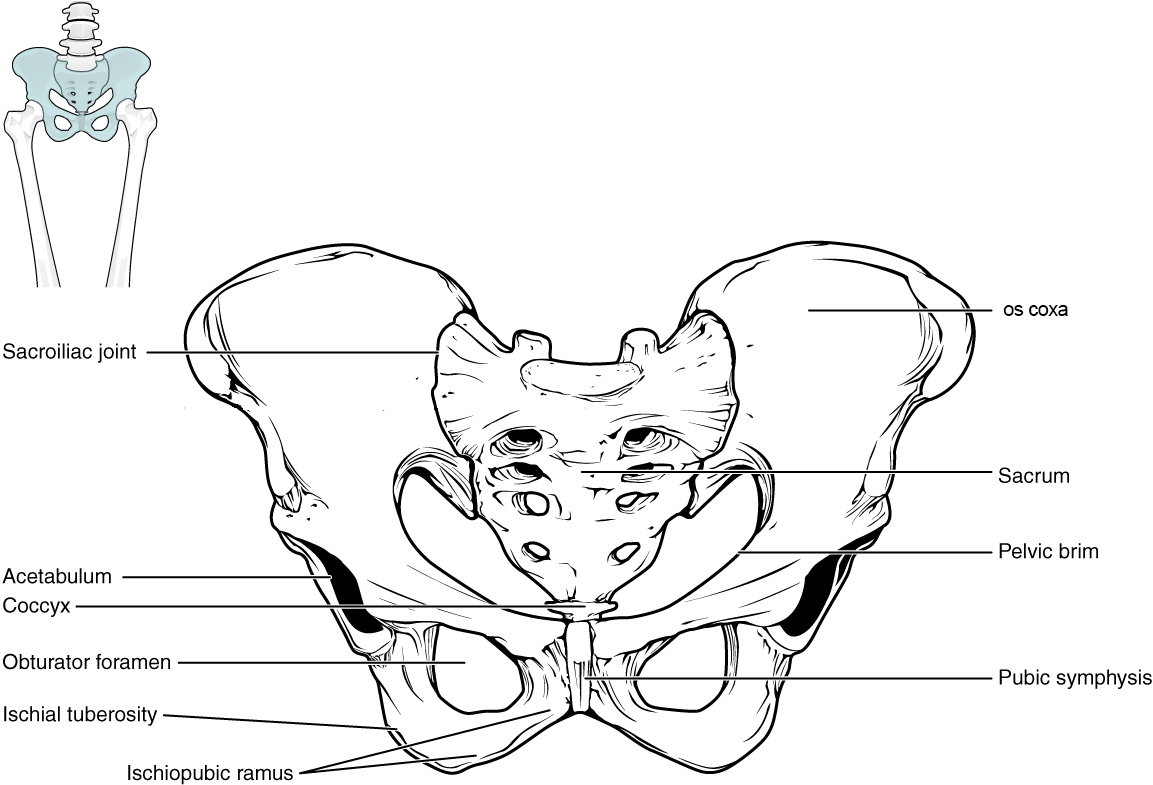
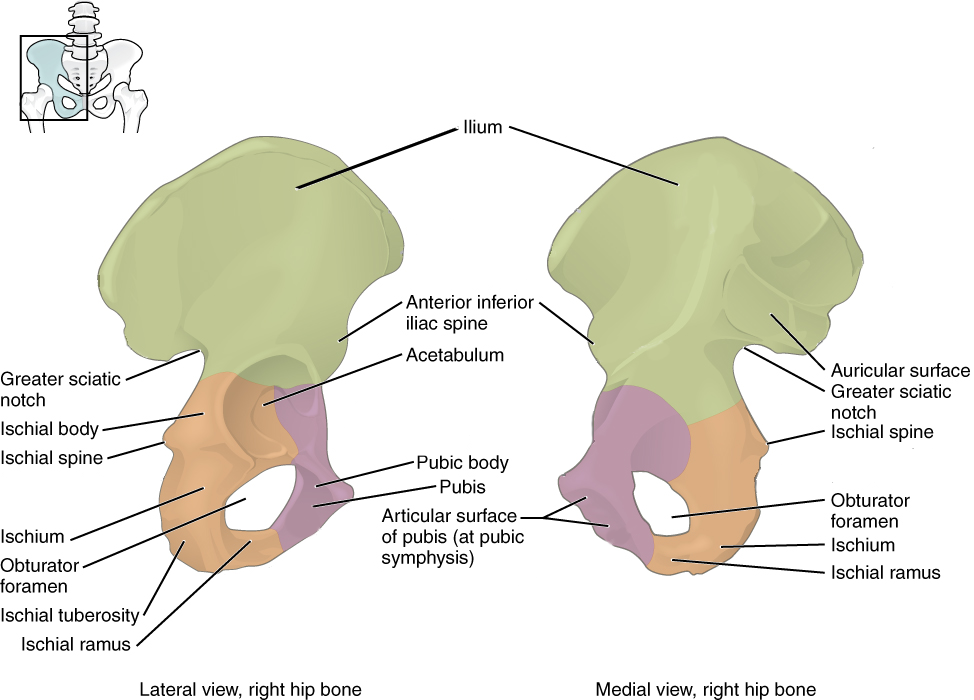
The pelvic girdle consists of the two os coxae and the sacrum that articulates with both, and it serves as the proximal base and anchor of the lower limb to the axial skeleton. Each os coxa comprises three bones that fuse together during growth: ilium, ischium, and pubis. These three bones fuse in a region called the acetabulum, which is the socket for the ball-and-socket hip joint (Figure A.36).1
The pelvis has several important functions. Its primary role is to support the weight of the upper body when sitting and to transfer this weight to the lower limbs when standing. It serves as an attachment point for trunk and lower limb muscles, and also protects the internal pelvic organs. When standing in the anatomical position, the pelvis is tilted anteriorly. In this position, the anterior superior iliac spines and the pubic tubercles lie in the same vertical plane, and the anterior (internal) surface of the sacrum faces forward and downward.2
Ilium
The ilium, the flared superior portion of the pelvis, is the largest bone of the os coxa and serves as a major site of attachments for muscles from the abdomen, back, and lower limb. The ilium has several important features including the auricular surface, the surface where the ilium articulates with the sacrum. The auricular surface is used to estimate age at death as the surface progressively deteriorates with increasing age to appear coarse and porous. The greater sciatic notch is a large notch in the ilium that allows for several structures to leave the pelvis and enter the lower extremity, including the sciatic nerve. In females, the notch tends to be symmetrical whereas in males it tends to curve posteriorly.1
Ischium
The ischium forms the posterior and inferior portion of the os coxa. There are two significant projections of note on the ischium: the ischial spine and tuberosity. The ischial spine is the attachment point for a major pelvic ligament and is located inferior to the greater sciatic notch of the ilium. The ischial tuberosity is the proximal attachment site for the hamstring muscles of the lower limb.1
Pubis
The anterior and medial portions of the os coxa are formed by the pubis. The pubis is a useful bone with which to sex a skeleton in a forensic context. The body is the superior and medial portion of the pubis (Figure A.37). The body tends to be rectangular in cross-section in females and triangular in males. The bony projection that unites the ischium and pubis anteriorly is called the ischiopubic ramus. Females tend to display a thin and sharp ramus on the medial surface while the surface in males tends to be broad and blunt. The joint that unites the two pubic bones in the front of the pelvis is called the pubic symphysis, which is a structure commonly used in age estimation. In young adults, the surface is billowed, but it transitions to being smooth and porous with increasing age. The subpubic concavity is a depression inferior to the ischiopubic ramus. Females tend to exhibit a concavity while males tend to be straight. Finally, the large opening encircled by the pubis and ischium is called the obturator foramen. The shape of the foramen in females has been described as triangular while it is more likely to appear oval in males.1
Bones of the Lower Limb
Like the upper limb, the lower limb is divided into three regions. The thigh is that portion of the lower limb located between the hip joint and knee joint. The leg is specifically the region between the knee joint and the ankle joint. Distal to the ankle is the foot. The lower limb contains 30 bones. These are the femur, patella, tibia, fibula, tarsal bones, metatarsal bones, and phalanges. The femur is the single bone of the thigh. The patella is the kneecap and articulates with the distal femur. The tibia is the larger, weight-bearing bone located on the medial side of the leg, and the fibula is the thin bone of the lateral leg. The bones of the foot are divided into three groups. The posterior portion of the foot is formed by a group of seven bones, each of which is known as a tarsal bone, whereas the mid-foot contains five elongated bones, each of which is a metatarsal bone. The toes contain 14 small bones, each of which is a phalanx bone of the foot.2
Femur
The femur, or thigh bone, is the single bone of the thigh region (Figure A. 38). It is the longest and strongest bone of the body, and accounts for approximately one-quarter of a person’s total height. The rounded, proximal end is the head of the femur, which articulates with the acetabulum of the hip bone to form the hip joint. The fovea capitis is a minor indentation on the medial side of the femoral head that serves as the site of attachment for the ligament of the head of the femur. This ligament spans the femur and acetabulum, but is weak and provides little support for the hip joint. It does, however, carry an important artery that supplies the head of the femur.2
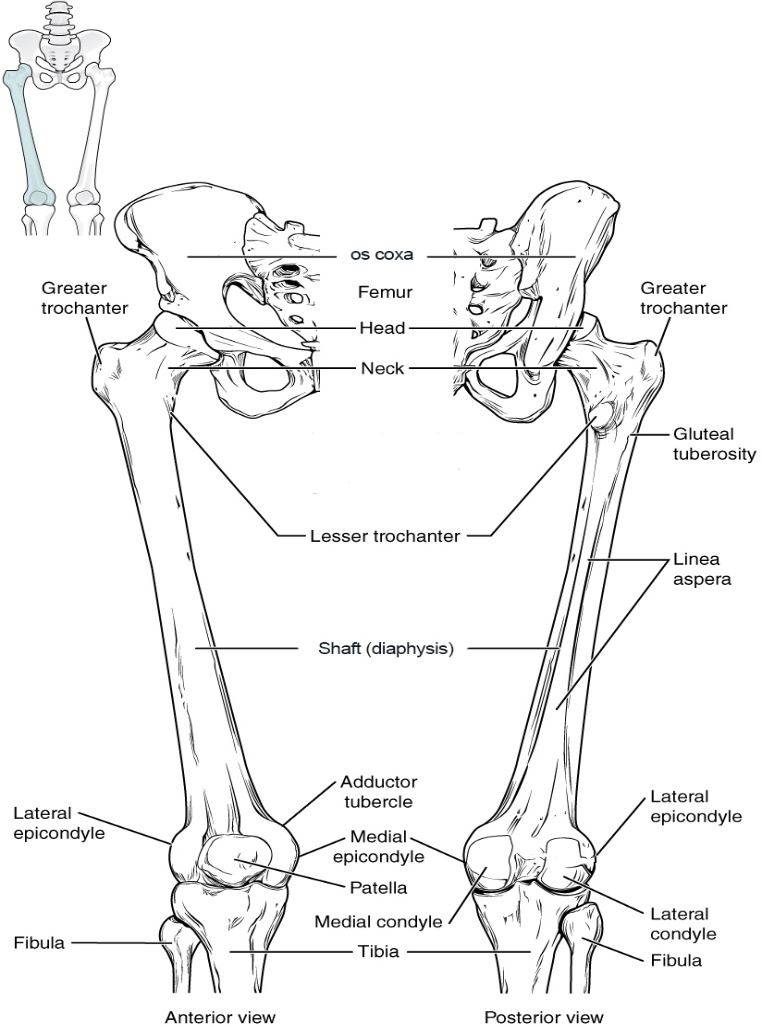
The narrowed region below the head is the neck of the femur. This is a common area for fractures of the femur. The greater trochanter is the large, upward, bony projection located above the base of the neck. Multiple muscles that act across the hip joint attach to the greater trochanter, which, because of its projection from the femur, gives additional leverage to these muscles. The greater trochanter can be felt just under the skin on the lateral side of your upper thigh. The lesser trochanter is a small, bony prominence that lies on the medial aspect of the femur, just below the neck. A single, powerful muscle attaches to the lesser trochanter.2
The distal end of the femur has medial and lateral bony expansions. On the lateral side, the smooth portion that covers the distal and posterior aspects of the lateral expansion is the lateral condyle of the femur. The roughened area on the outer, lateral side of the condyle is the lateral epicondyle of the femur. Similarly, the smooth region of the distal and posterior medial femur is the medial condyle of the femur, and the irregular outer, medial side of this is the medial epicondyle of the femur. The lateral and medial condyles articulate with the tibia to form the knee joint. The epicondyles provide attachment for muscles and supporting ligaments of the knee. Posteriorly, the medial and lateral condyles are separated by a deep depression called the intercondylar fossa. Anteriorly, the smooth surfaces of the condyles join together to form a wide groove called the patellar surface, which provides for articulation with the patella bone. The combination of the medial and lateral condyles with the patellar surface gives the distal end of the femur a horseshoe (U) shape.2
Patella
The patella (kneecap) is largest sesamoid bone of the body (see Figure A. 38). A sesamoid bone is a bone that is incorporated into the tendon of a muscle where that tendon crosses a joint. The sesamoid bone articulates with the underlying bones to prevent damage to the muscle tendon due to rubbing against the bones during movements of the joint. The patella is found in the tendon of the quadriceps femoris muscle, the large muscle of the anterior thigh that passes across the anterior knee to attach to the tibia. The patella articulates with the patellar surface of the femur and thus prevents rubbing of the muscle tendon against the distal femur. The patella also lifts the tendon away from the knee joint, which increases the leverage power of the quadriceps femoris muscle as it acts across the knee. The patella does not articulate with the tibia.2
Tibia
The tibia (shin bone) is the medial bone of the leg and is larger than the fibula, with which it is paired (Figure A. 39). The tibia is the main weight-bearing bone of the lower leg and the second longest bone of the body, after the femur. he proximal end of the tibia is greatly expanded. The two sides of this expansion form the medial condyle of the tibia and the lateral condyle of the tibia. The tibia does not have epicondyles. The top surface of each condyle is smooth and flattened. These areas articulate with the medial and lateral condyles of the femur to form the knee joint. Between the articulating surfaces of the tibial condyles is the intercondylar eminence, an irregular, elevated area that serves as the inferior attachment point for two supporting ligaments of the knee.2
The tibial tuberosity is an elevated area on the anterior side of the tibia, near its proximal end. It is the final site of attachment for the muscle tendon associated with the patella. A small ridge running down the lateral side of the tibial shaft is the interosseous border of the tibia. This is for the attachment of the interosseous membrane of the leg, the sheet of dense connective tissue that unites the tibia and fibula bones.2
The large expansion found on the medial side of the distal tibia is the medial malleolus (“little hammer”). This forms the large bony bump found on the medial side of the ankle region. Both the smooth surface on the inside of the medial malleolus and the smooth area at the distal end of the tibia articulate with the talus bone of the foot as part of the ankle joint. On the lateral side of the distal tibia is a wide groove called the fibular notch. This area articulates with the distal end of the fibula, forming the distal tibiofibular joint.2
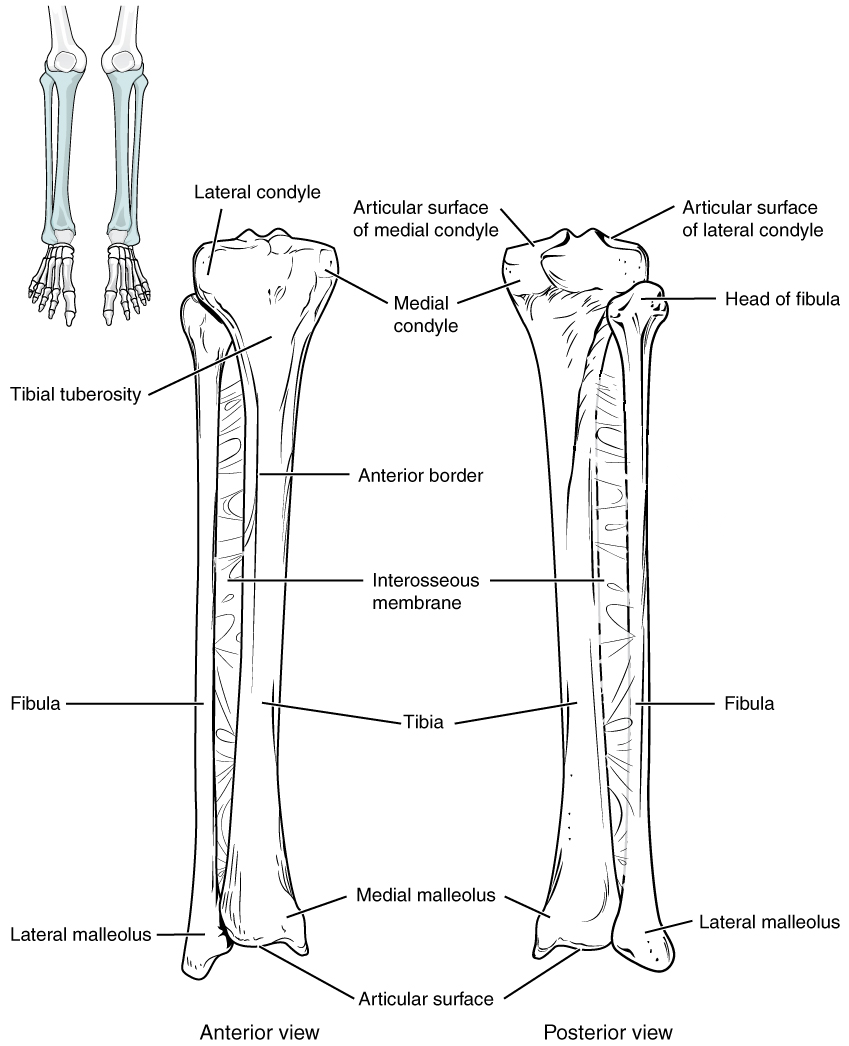
Fibula
The fibula is the slender bone located on the lateral side of the leg (see Figure A. 39). The fibula does not bear weight. It serves primarily for muscle attachments and thus is largely surrounded by muscles. Only the proximal and distal ends of the fibula can be palpated.2
The head of the fibula is the small, knob-like, proximal end of the fibula. It articulates with the inferior aspect of the lateral tibial condyle, forming the proximal tibiofibular joint. The thin shaft of the fibula has the interosseous border of the fibula, a narrow ridge running down its medial side for the attachment of the interosseous membrane that spans the fibula and tibia. The distal end of the fibula forms the lateral malleolus, which forms the easily palpated bony bump on the lateral side of the ankle. The deep (medial) side of the lateral malleolus articulates with the talus bone of the foot as part of the ankle joint. The distal fibula also articulates with the fibular notch of the tibia.2
Tarsals
There are seven tarsal bones that comprise the ankle (Figure A.40). The talus is the most superior of the tarsals, and it articulates with the distal tibia and distal fibula superiorly and with the calcaneus inferiorly. The calcaneus is the heel of the foot; it is the largest of the tarsals. On the posterior-most aspect of the calcaneus is the calcaneal tuberosity, which is the attachment site for the Achilles tendon of the posterior leg. Distal to the talus is the medially positioned navicular, the three cuneiform bones (medial, intermediate, and lateral), and the laterally positioned cuboid.1
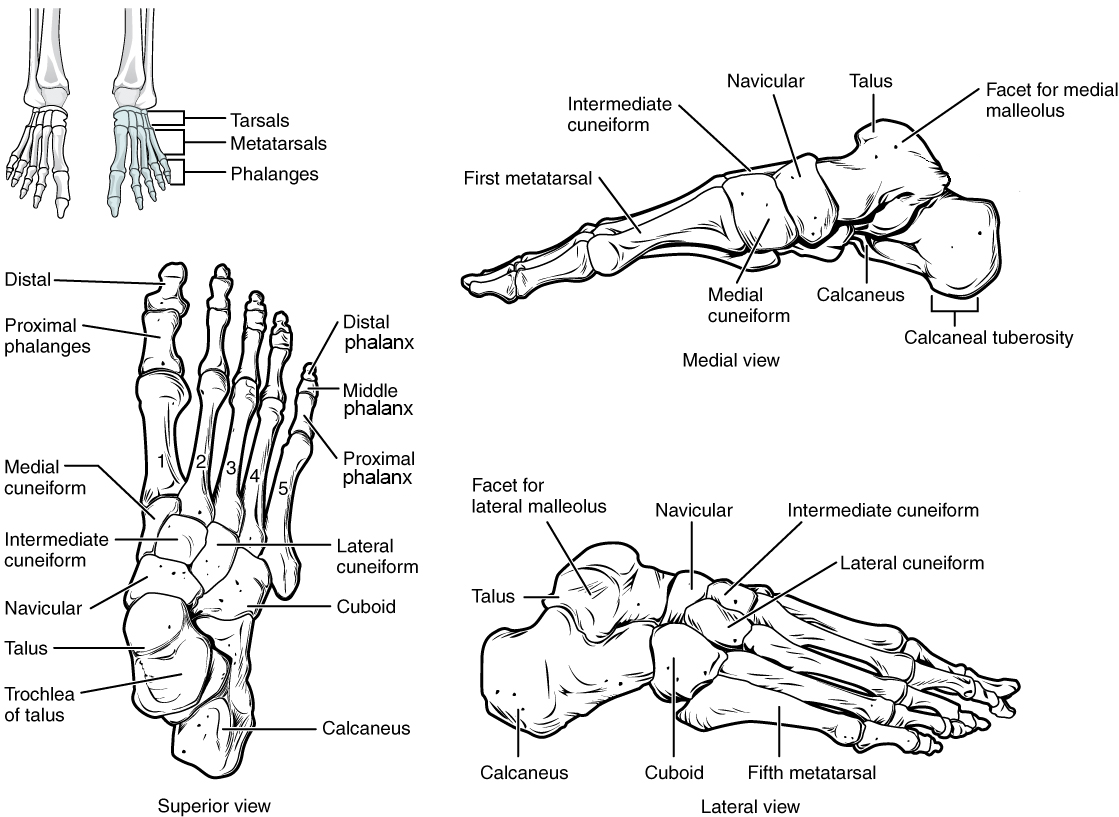
Metatarsal Bones
The anterior half of the foot is formed by the five metatarsal bones, which are located between the tarsal bones of the posterior foot and the phalanges of the toes (see Figure A. 40). These elongated bones are numbered 1–5, starting with the medial side of the foot. The first metatarsal bone is shorter and thicker than the others. The second metatarsal is the longest. The base of the metatarsal bone is the proximal end of each metatarsal bone. These articulate with the cuboid or cuneiform bones. The base of the fifth metatarsal has a large, lateral expansion that provides for muscle attachments. This expanded base of the fifth metatarsal can be felt as a bony bump at the midpoint along the lateral border of the foot. The expanded distal end of each metatarsal is the head of the metatarsal bone. Each metatarsal bone articulates with the proximal phalanx of a toe to form a metatarsophalangeal joint. The heads of the metatarsal bones also rest on the ground and form the ball (anterior end) of the foot.2
Phalanges
The toes contain a total of 14 phalanx bones (phalanges), arranged in a similar manner as the phalanges of the fingers (see Figure A. 40). The toes are numbered 1–5, starting with the big toe (hallux). The big toe has two phalanx bones, the proximal and distal phalanges. The remaining toes all have proximal, middle, and distal phalanges. A joint between adjacent phalanx bones is called an interphalangeal joint.2
Joints
A joint, also called an articulation, is any place where adjacent bones or bone and cartilage come together (articulate with each other) to form a connection. Joints are classified both structurally and functionally. Structural classifications of joints take into account whether the adjacent bones are strongly anchored to each other by fibrous connective tissue or cartilage, or whether the adjacent bones articulate with each other within a fluid-filled space called a joint cavity. Functional classifications describe the degree of movement available between the bones, ranging from immobile, to slightly mobile, to freely moveable joints.2
In a fibrous joint, the adjacent bones are directly connected to each other by fibrous connective tissue, and thus the bones do not have a joint cavity between them. In a cartilaginous joint, the adjacent bones are united by cartilage, a tough but flexible type of connective tissue. These types of joints lack a joint cavity and involve bones that are joined together by either hyaline cartilage or fibrocartilage. Synovial joints are the most common type of joint in the body. A key structural characteristic for a synovial joint that is not seen at fibrous or cartilaginous joints is the presence of a joint cavity. This fluid-filled space is the site at which the articulating surfaces of the bones contact each other. Also, unlike fibrous or cartilaginous joints, the articulating bone surfaces at a synovial joint are not directly connected to each other with fibrous connective tissue or cartilage. This gives the bones of a synovial joint the ability to move smoothly against each other, allowing for increased joint mobility.2
References:
1. Jason M. Organ and Jessica N. Byram, “Osteology” In Explorations, ed. Beth Shook, Katie Nelson, Kelsie Aguilera and Lara Braff (Arlington: American Anthropological Association, 2019). https://pressbooksdev.oer.hawaii.edu/explorationsbioanth/chapter/osteology/.
2. Layci Harrison, Anatomical Basis of Injury (Houston: University of Houston, 2019). https://uhlibraries.pressbooks.pub/atpanatomy/front-matter/about-this-book/.
Figure Attributions:
Figure A.1 Regions of the Human Body (Anatomy & Physiology, Figure 1.12) by OpenStax has been modified (labels removed) and is used under a CC BY 4.0 License.
Figure A.2 Planes of the Body (Anatomy & Physiology, Figure 1.14) by OpenStax has been modified (some labels modified) and is used under a CC BY 4.0 License.
Figure A.3 Directional Terms Applied to the Human Body (Anatomy & Physiology, Figure 1.13) by OpenStax is used under a CC BY 4.0 License.
Figure A.4 Anatomy of a Long Bone (Anatomy & Physiology, Figure 6.7) by OpenStax has been modified (some labels modified or removed) and is used under a CC BY 4.0 License.
Figure A.5 Bone Cells (Anatomy & Physiology, Figure 6.11) by OpenStax is used under a CC BY 4.0 License.
Figure A.6 Classifications of Bones (Anatomy & Physiology, Figure 6.6) by OpenStax is used under a CC BY 4.0 License.
Figure A.7 Intramembranous Ossification (Anatomy & Physiology, Figure 6.16) by OpenStax has been modified (some labels modified or removed) and is used under a CC BY 4.0 License.
Figure A.8 Endochondral Ossification (Anatomy & Physiology, Figure 6.17) by OpenStax has been modified (some labels modified or removed) and is used under a CC BY 4.0 License.
Figure A.9 Pathways in Calcium Homeostasis (Anatomy & Physiology, Figure 6.24) by OpenStax is used under a CC BY 4.0 License.
Figure A.10 Axial and Appendicular Skeleton (Anatomy & Physiology, Figure 7.2) by OpenStax is used under a CC BY 4.0 License.
Figure A.11 Parts of the Skull (Anatomy & Physiology, Figure 7.3) by OpenStax has been modified (some labels modified or removed) and is used under a CC BY 4.0 License.
Figure A.12 Anterior View of Skull (Anatomy & Physiology, Figure 7.4) by OpenStax has been modified (some labels removed) and is used under a CC BY 4.0 License.
Figure A.13 Lateral View of Skull (Anatomy & Physiology, Figure 7.5) by OpenStax has been modified (some labels removed) and is used under a CC BY 4.0 License.
Figure A.14 Temporal Bone (Anatomy & Physiology, Figure 7.7) by OpenStax has been modified (some labels removed) and is used under a CC BY 4.0 License.
Figure A.15 External and Internal Views of Base of Skull (Anatomy & Physiology, Figure 7.8) by OpenStax has been modified (some labels modified or removed) and is used under a CC BY 4.0 License.
Figure A.16 Sphenoid Bone (Anatomy & Physiology, Figure 7.10) by OpenStax has been modified (some labels removed) and is used under a CC BY 4.0 License.
Figure A.17 Ethmoid Bone (Anatomy & Physiology, Figure 7.12) by OpenStax has been modified (some labels removed) and is used under a CC BY 4.0 License.
Figure A.18 Maxillary Bone (Anatomy & Physiology, Figure 7.14) by OpenStax has been modified (some labels modified or removed) and is used under a CC BY 4.0 License.
Figure A.19 Bones of the Orbit (Anatomy & Physiology, Figure 7.16) by OpenStax has been modified (some labels removed) and is used under a CC BY 4.0 License.
Figure A.20 Nasal Septum (Anatomy & Physiology, Figure 7.17) by OpenStax has been modified (some labels modified or removed) and is used under a CC BY 4.0 License.
Figure A.21 Lateral Wall of Nasal Cavity (Anatomy & Physiology, Figure 7.13) by OpenStax has been modified (some labels removed) and is used under a CC BY 4.0 License.
Figure A.22 Hyoid Bone (Anatomy & Physiology, Figure 7.19) by OpenStax has been modified (some labels removed) and is used under a CC BY 4.0 License.
Figure A.23 Isolated Mandible (Anatomy & Physiology, Figure 7.15) by OpenStax has been modified (some labels modified or removed) and is used under a CC BY 4.0 License.
Figure A.24 Parts of a Typical Vertebra (Anatomy & Physiology, Figure 7.23) by OpenStax has been modified (some labels removed) and is used under a CC BY 4.0 License.
Figure A.25 Cervical Vertebra (Anatomy & Physiology, Figure 7.25) by OpenStax has been modified (some labels removed) and is used under a CC BY 4.0 License.
Figure A.26 Rib Articulation in Thoracic Vertebrae (Anatomy & Physiology, Figure 7.27) by OpenStax has been modified (some labels removed) and is used under a CC BY 4.0 License.
Figure A.27 Lumbar Vertebrae (Anatomy & Physiology, Figure 7.28) by OpenStax is used under a CC BY 4.0 License.
Figure A.28 Sacrum and Coccyx (Anatomy & Physiology, Figure 7.29) by OpenStax has been modified (some labels removed) and is used under a CC BY 4.0 License.
Figure A.29 Vertebral Column (Anatomy & Physiology, Figure 7.20) by OpenStax has been modified (some labels modified or removed) and is used under a CC BY 4.0 License.
Figure A.30 Thoracic Cage (Anatomy & Physiology, Figure 7.32) by OpenStax has been modified (some labels modified or removed) and is used under a CC BY 4.0 License.
Figure A.31 Pectoral Girdle (Anatomy & Physiology, Figure 8.3) by OpenStax has been modified (some labels modified or removed) and is used under a CC BY 4.0 License.
Figure A.32 Scapula (Anatomy & Physiology, Figure 8.4) by OpenStax has been modified (some labels modified or removed) and is used under a CC BY 4.0 License.
Figure A.33 Humerus and Elbow Joint (Anatomy & Physiology, Figure 8.5) by OpenStax has been modified (some labels modified or removed) and is used under a CC BY 4.0 License.
Figure A.34 Ulna and Radius (Anatomy & Physiology, Figure 8.6) by OpenStax has been modified (some labels removed) and is used under a CC BY 4.0 License.
Figure A.35 Bones of the Wrist and Hand (Anatomy & Physiology, Figure 8.7) by OpenStax has been modified (some labels removed) and is used under a CC BY 4.0 License.
Figure A.36 Pelvis (Anatomy & Physiology, Figure 8.12) by OpenStax has been modified (some labels modified or removed) and is used under a CC BY 4.0 License.
Figure A.37 The Hip Bone (Anatomy & Physiology, Figure 8.13) by OpenStax has been modified (some labels removed) and is used under a CC BY 4.0 License.
Figure A.38 Femur and Patella (Anatomy & Physiology, Figure 8.16) by OpenStax has been modified (some labels modified or removed) and is used under a CC BY 4.0 License.
Figure A.39 Tibia and Fibula (Anatomy & Physiology, Figure 8.18) by OpenStax has been modified (one label removed) and is used under a CC BY 4.0 License.
Figure A.40 Bones of the Foot (Anatomy & Physiology, Figure 8.19) by OpenStax has been modified (some labels modified or removed) and is used under a CC BY 4.0 License.
